Case Presentation
Presenting Complaint
Tom Morris is a 50 year old self-employed plumber and shop owner. He is 172cm tall, 85 kg in weight and is in good physical shape. Mr. Morris presented to the emergency department following his participation in the Dublin City Marathon which he was unable to complete due to a number of major in-race complications.
Prior to lining up at the races start Mr Morris's training had been consistent in its incorporation of regular gym sessions. His pre-race preparations did not however include any "Carbohydrate loading" but instead comprised of only a fish and chips take out meal the night before the race.
On race day Mr. Morris managed to run to the 18 km mark without experiencing any hassle. He opted out of stopping at any of the drinks stations. From this point to the 29km mark he noticed the onset of a progressing ache in his legs and had been gritting his teeth. At this point Mr. Morris's legs became so heavy that he could no longer raise them.
Cold and light headed, Mr. Morris was reduced to a mere walk at 30km and finally collapsed to the ground in a confused and disorientated state with black spots in his visual field. An ambulance volunteer initiated a vitals check measuring Tom's pulse and blood pressure, and subsequently providing him with an insulating 'space' blanket. Once the vitals were reported normal TM was given an energy drink and began to get up. It transpired that he had incurred an ankle sprain due to his foot inverting during his collapse.
ED and Triage Assesment
A registrar-ordered X-Ray revealed that a fracture was not sustained to the ankle, however post-radiography, the status of ankle inversion and lateral ligament damage was ascribed to Mr. Morris with local supportive measures being recommended.
Tom Morris is a 50 year old self-employed plumber and shop owner. He is 172cm tall, 85 kg in weight and is in good physical shape. Mr. Morris presented to the emergency department following his participation in the Dublin City Marathon which he was unable to complete due to a number of major in-race complications.
Prior to lining up at the races start Mr Morris's training had been consistent in its incorporation of regular gym sessions. His pre-race preparations did not however include any "Carbohydrate loading" but instead comprised of only a fish and chips take out meal the night before the race.
On race day Mr. Morris managed to run to the 18 km mark without experiencing any hassle. He opted out of stopping at any of the drinks stations. From this point to the 29km mark he noticed the onset of a progressing ache in his legs and had been gritting his teeth. At this point Mr. Morris's legs became so heavy that he could no longer raise them.
Cold and light headed, Mr. Morris was reduced to a mere walk at 30km and finally collapsed to the ground in a confused and disorientated state with black spots in his visual field. An ambulance volunteer initiated a vitals check measuring Tom's pulse and blood pressure, and subsequently providing him with an insulating 'space' blanket. Once the vitals were reported normal TM was given an energy drink and began to get up. It transpired that he had incurred an ankle sprain due to his foot inverting during his collapse.
ED and Triage Assesment
A registrar-ordered X-Ray revealed that a fracture was not sustained to the ankle, however post-radiography, the status of ankle inversion and lateral ligament damage was ascribed to Mr. Morris with local supportive measures being recommended.
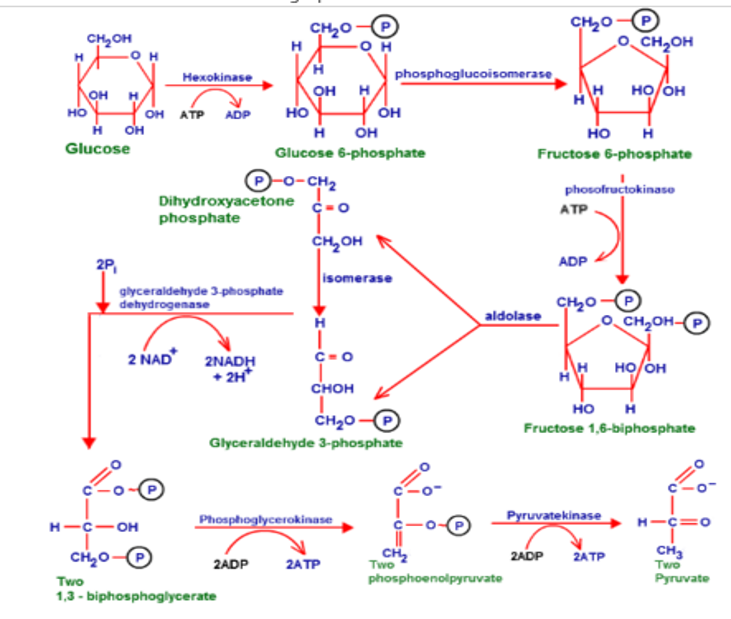
Explain how muscles derive energy from different fuels.
⇨ Organs and their fuel storage
Liver
The liver has the capacity to hold roughly ~100g
Skeletal Muscle
Skeletal muscle is controlled by feedback -mediated inhibition of glucose synthase and has the capacity to hold roughly 500g of glycogen.
Blood
Has a random plasma glucose of below 200mg/dL or 1.1mmol/L
Brain
Has a strong reliance on glucose but can alternatively use ketone bodies as a form of fuel in situations where glucose is absent.
The brain has a very small amount of glycogen present in association with the astrocyte cells.
MCFA and Lactate can also be used to a lesser extent by neuronal cells as an energy source.
Fat/Lipid
Human adipose tissue contains about 87% of the body's lipid reserve.
Free fatty acids are liberated from lipoproteins by lipoprotein lipase (LPL) and subsequently enter adipocyte for storage purposes.
FFAs are reassembled into triglycerides through esterification of glycerol.
An Insulin ↑ - brings FFA into adipocytes
A Lipase ↑ - brings FFA out from adipocytes
The liver has the capacity to hold roughly ~100g
Skeletal Muscle
Skeletal muscle is controlled by feedback -mediated inhibition of glucose synthase and has the capacity to hold roughly 500g of glycogen.
Blood
Has a random plasma glucose of below 200mg/dL or 1.1mmol/L
Brain
Has a strong reliance on glucose but can alternatively use ketone bodies as a form of fuel in situations where glucose is absent.
The brain has a very small amount of glycogen present in association with the astrocyte cells.
MCFA and Lactate can also be used to a lesser extent by neuronal cells as an energy source.
Fat/Lipid
Human adipose tissue contains about 87% of the body's lipid reserve.
Free fatty acids are liberated from lipoproteins by lipoprotein lipase (LPL) and subsequently enter adipocyte for storage purposes.
FFAs are reassembled into triglycerides through esterification of glycerol.
An Insulin ↑ - brings FFA into adipocytes
A Lipase ↑ - brings FFA out from adipocytes