Case Summary
Case Summary
- An arthroscopy confirms that Mr. Lawlor had most of his medial meniscus removed and there is damage to his articular cartilage, especially on the left. Dr. Burke decides there is little to do for his knees, but has recommended that he give up jogging and replace it with non-weight bearing exercise.
Describe the factors leading to the development of osteoarthritis and describe its consequences.
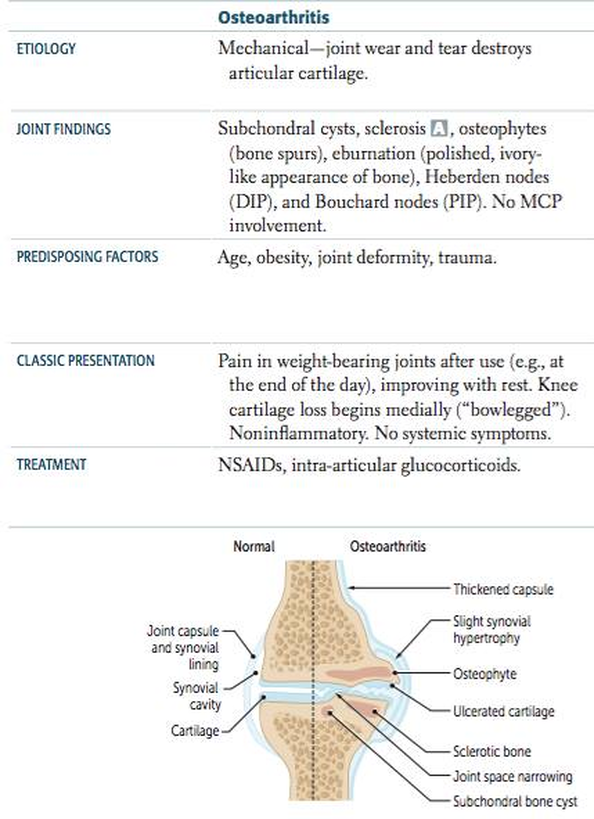
- Non-inflammatory joint disease with progressive degeneration of articular cartilage (weight bearing joints – femoral head of knee and lumbar vertebrae)
- Primary causes: Old age
- Secondary causes: Meniscal injuries (PBL case), obesity, trauma, neuropathic joint, Osteochondritis dissecans (cracks form in articular cartilage and underlying bone), hemochromatosis type 1 (increased iron absorption).
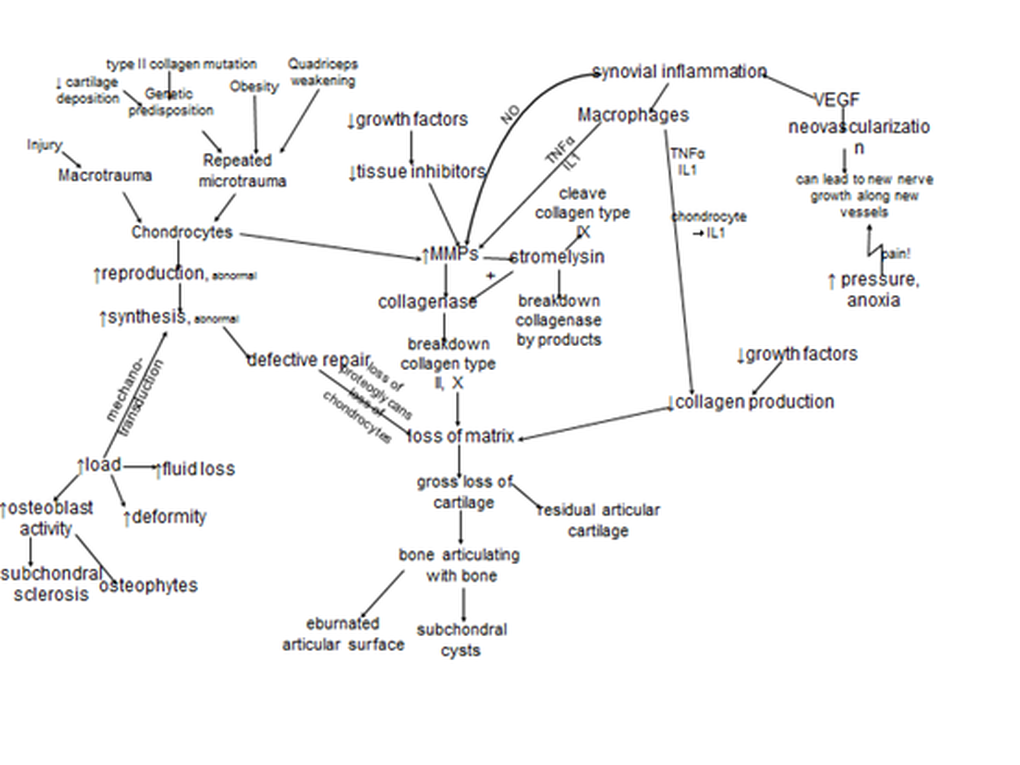
- Articular cartilage has proteoglycans which provide elasticity and type 2 collagen for strength
- IL-1 & TNF-α activate metalloproteinases:
- which reduce the proteoglycan content of the articular cartilage thereby increaseing water content of cartilage which in turn reduces resistance to pressure and leads to increased wear and tear
- degradation of articular collagen ultimately manifests as an overall degredation of the articular cartilage
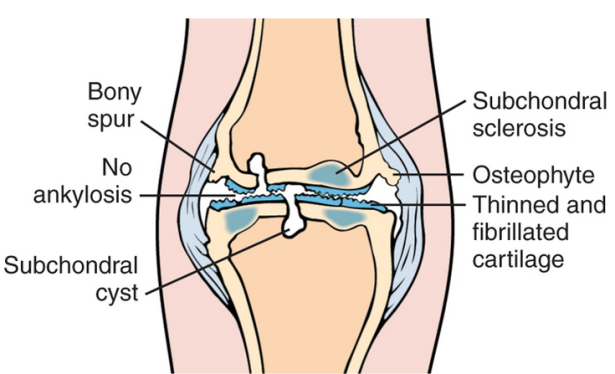
LOSS: Loss of joint of joint space Osteophytes Subchondral sclerosis Subchondral cysts |
|
|
Disease Signs and Symptoms
Localised Disease (specific to one joint);
|
|
Describe and explain the non-pharmacological and pharmacological therapy of lower limb osteoarthritis and sports injuries.
Non-pharm Mgmt.
Pharm: Short doses of analgesics, NSAIDS – to be used intermittently, Intra-articular corticosteroid injections – short-term relief from effusion
- Treat the symptoms and disability, not radiologic appearance
- Depression and poor quadriceps strength are better predictors of pain than x-ray severity
- Weight loss, Exercises for strength and stability, Hydrotherapy helps in lower limb OA, acupuncture has shown to help, Local heat, ice packs and massage, Insoles for shoes on the contralateral side to the affected lower limb joint are useful
Pharm: Short doses of analgesics, NSAIDS – to be used intermittently, Intra-articular corticosteroid injections – short-term relief from effusion
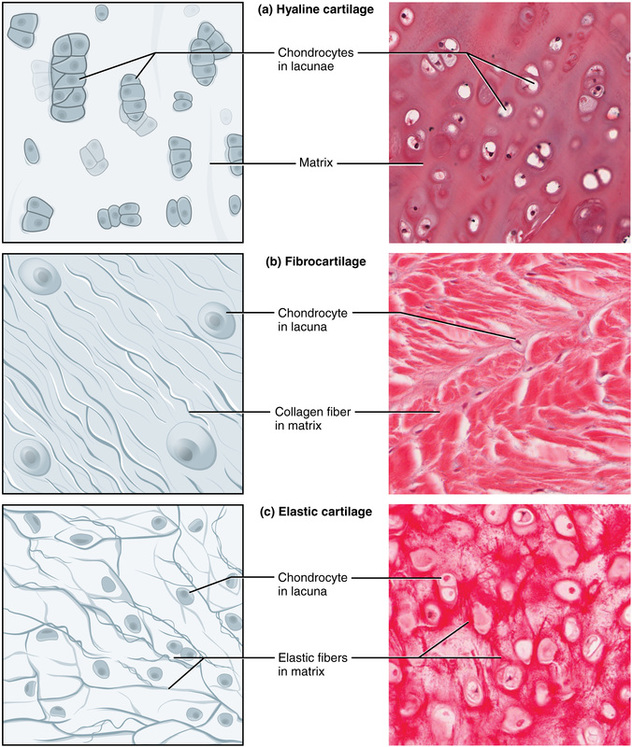
Describe the microscopic structure and properties of different types of cartilage.
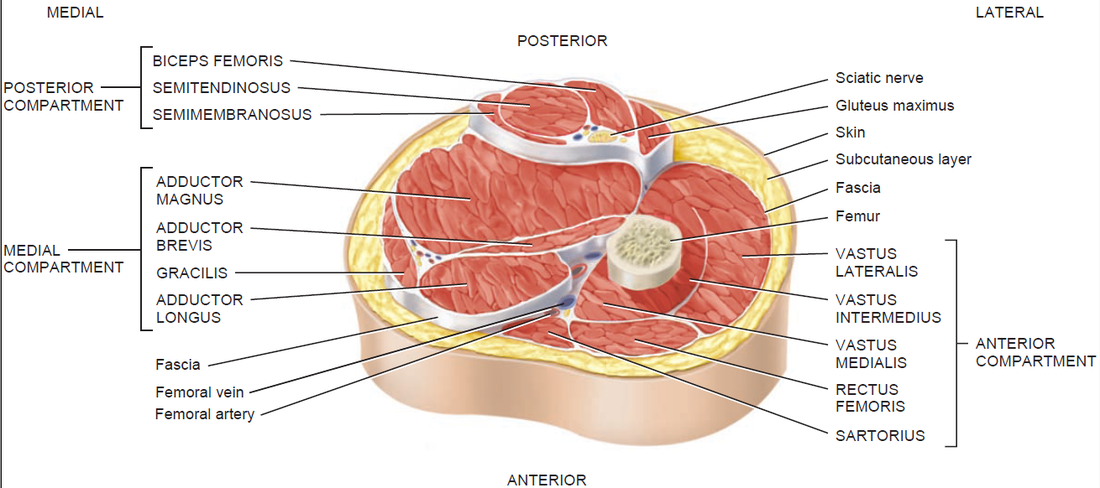
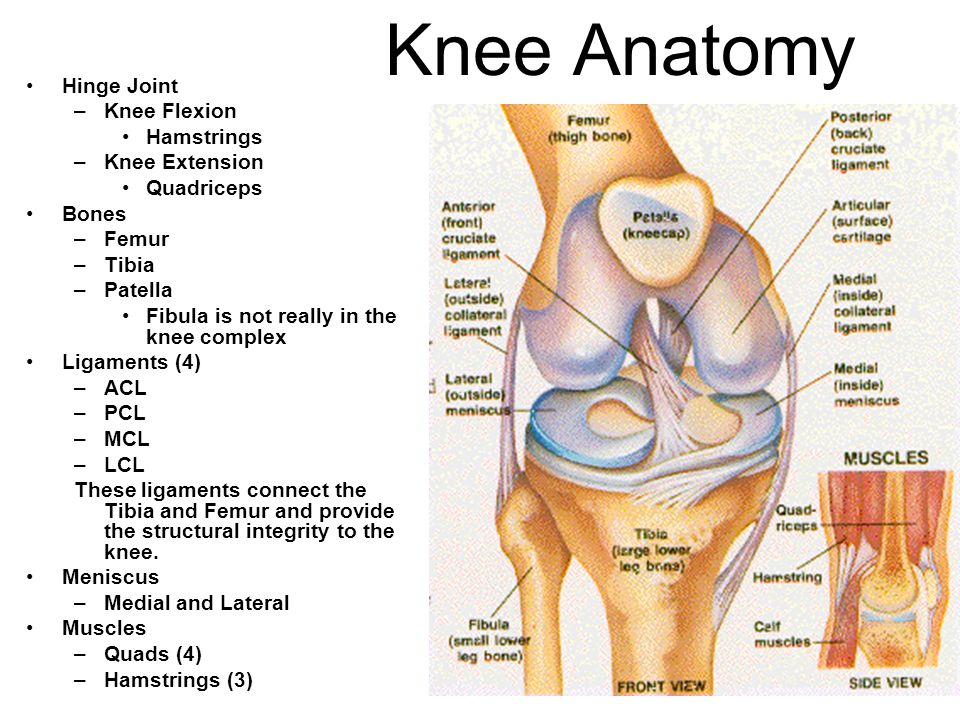
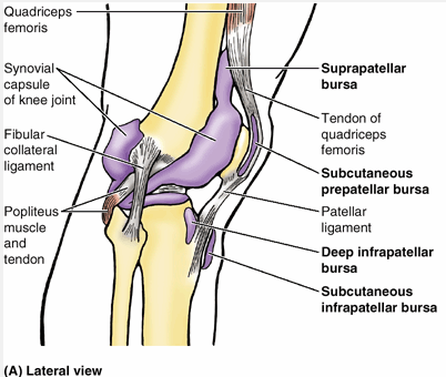
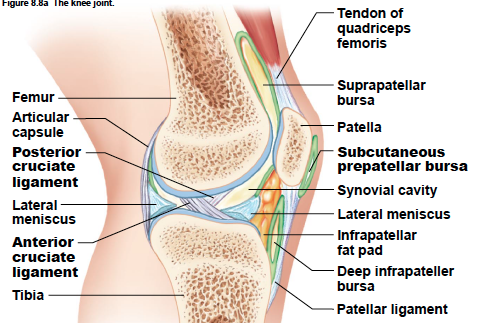
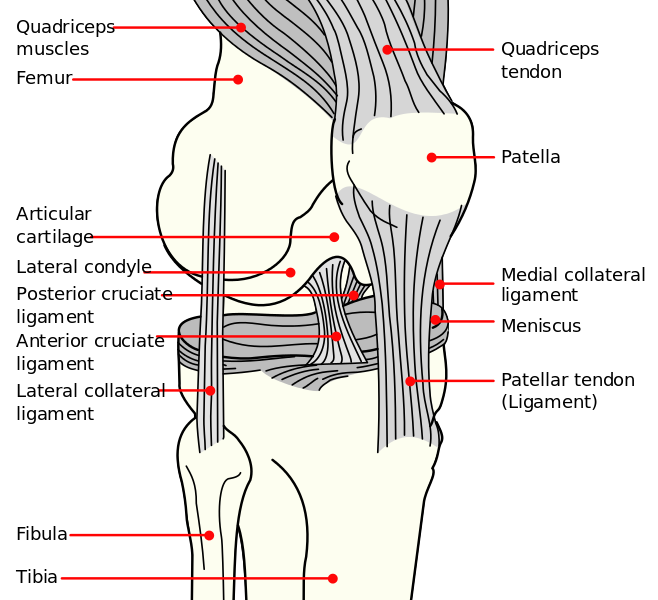
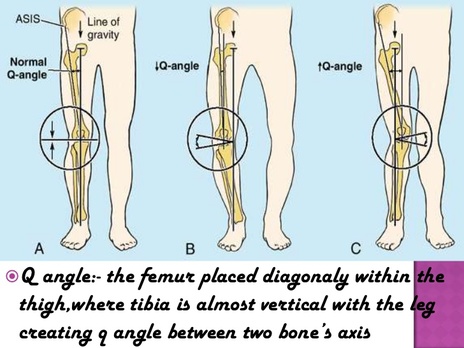
Identify the major skeletal structures of the lower limb with particular emphasis on the knee.
|
|
|
|
|
The Menisci
BIOMECHANICS
The major meniscal functions are to:
The major meniscal functions are to:
- Provide articular cartilage lubrication thus facilitating joint gliding and to
- Distribute stress across the knee during weight bearing, provide shock absorption and serve as secondary joint stabilizers.
- Other functions of the menisci are to provide articular cartilage lubrication thus facilitating joint gliding
|
|
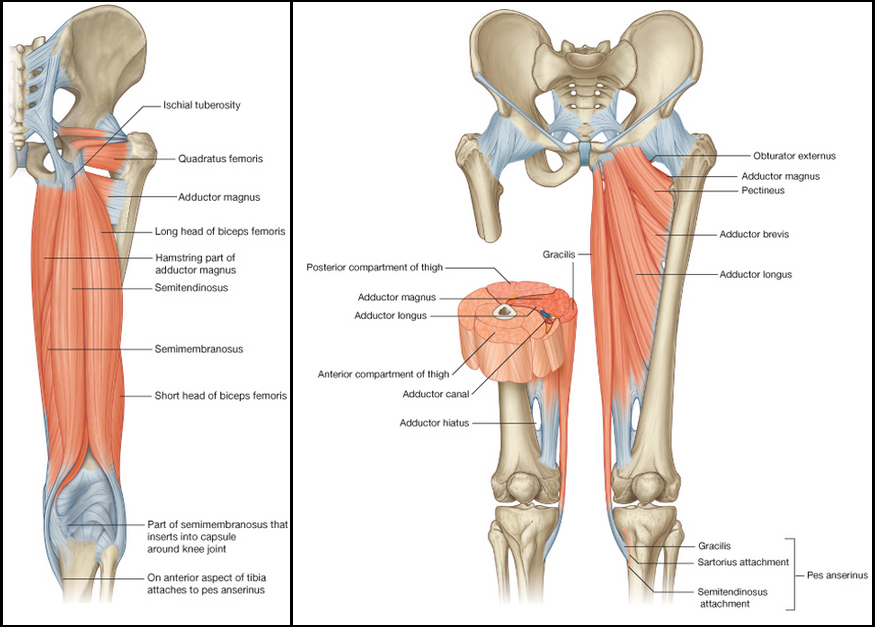
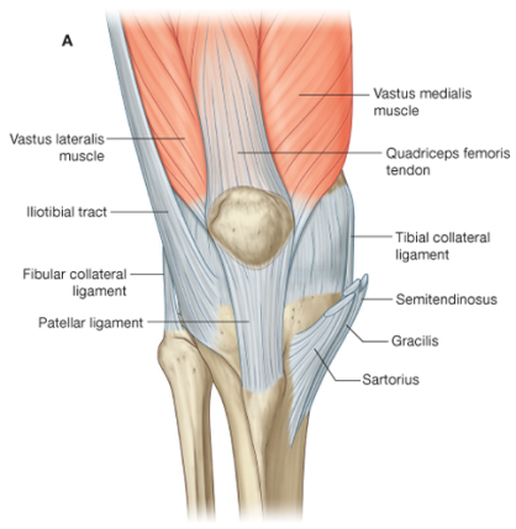
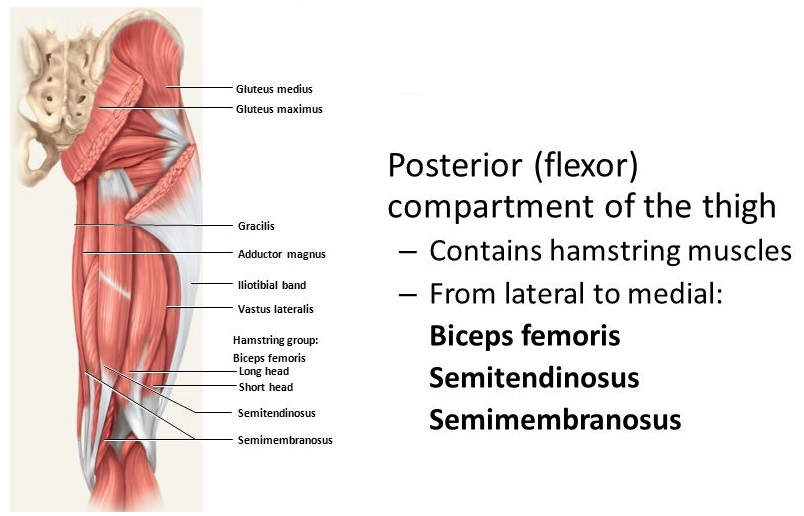
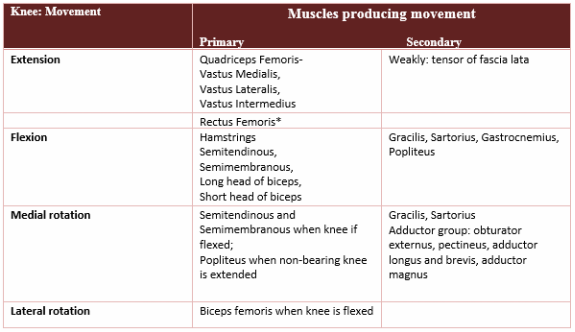
Identify the muscles acting on the knee, and describe their functions and innervation.
|
|
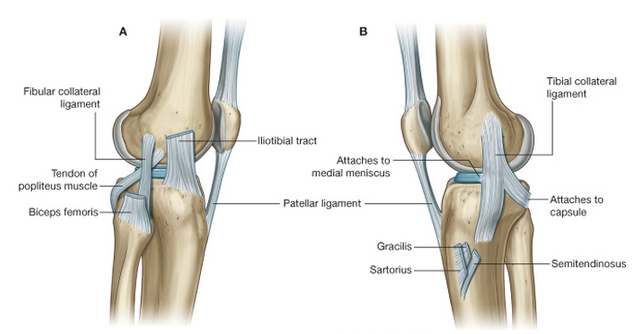
Describe the structure and movements of the knee, ankle and foot joints, including the organisation and functions of the ligaments.
Muscles and GAIT cycle
|
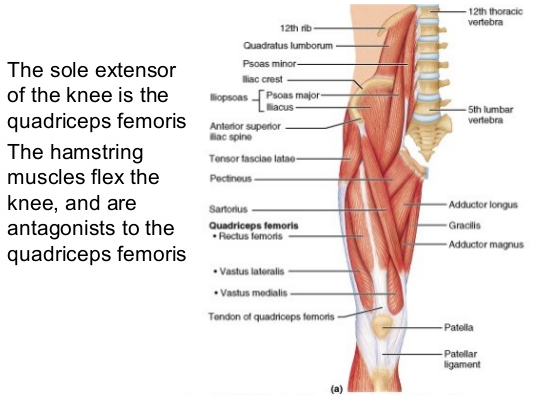
Muscle that extends the knee - Quadriceps
Parts of Qceps = Vastus lateralis, intermedius and medialis *Rectus femoris Its position creates too acute of an angle and it is too superficial to extend the Knee, Instead it is said to flex the hip In ordinary locomotion when do you flex the hip? As you go from pre-swing to early swing your hip flexors are active MOMENTUM extends the knee in the swing phase The quadriceps contract just before Initial contact (heel strike) |
Mobility and strength of the knee.
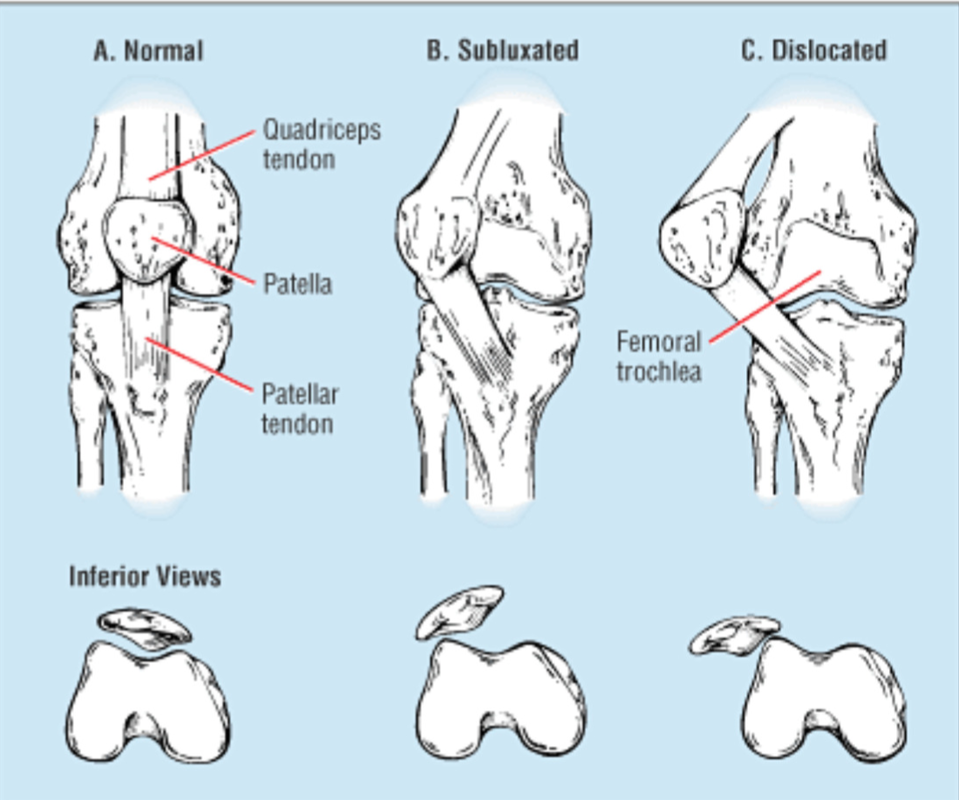
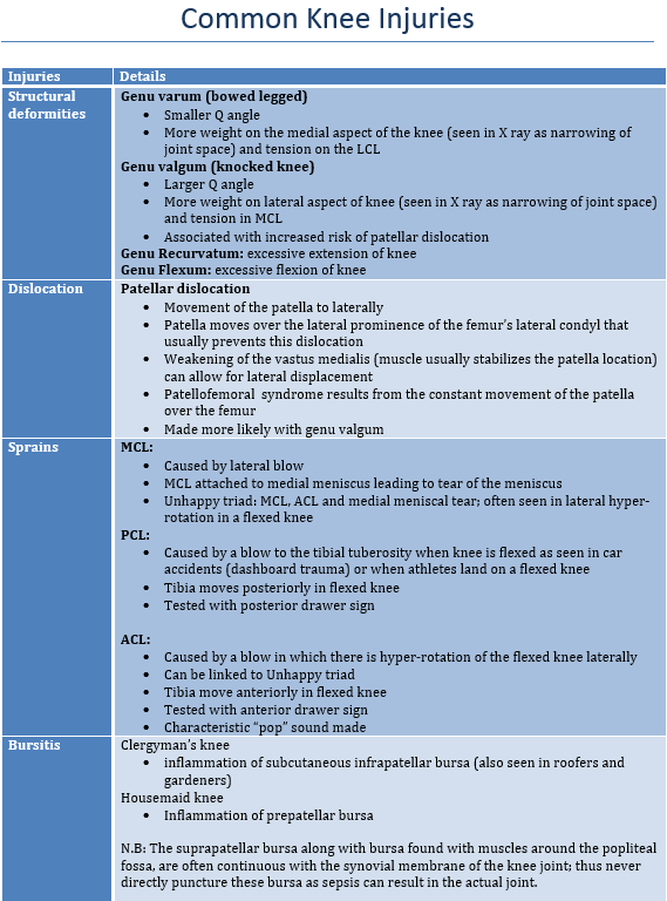
Describe the most common injuries to the knee and ankle and their causes.
|
|
Pharmacological and Non-pharmacological management of OA
kumar and clarke and almostadoctor.com
Sports injuries RICE – rest, ice , compression and elevation
NSAIDs are debatable regarding inflammation as part of healing
Surgery
OA
Management
Main objective is to treat symptoms and disability not the radiological findings
Educate the patient
Sports injuries RICE – rest, ice , compression and elevation
NSAIDs are debatable regarding inflammation as part of healing
Surgery
OA
Management
Main objective is to treat symptoms and disability not the radiological findings
Educate the patient
|
Physical
Weight loss and exercise to strengthen muscles Hydrotherapy for lower limb Heat/ice packs Massage NSAIDs gel Walking stick Acupuncture for the knee |
Mx: Medication
Balance benefits and side effects 1st step paracetemaol 2nd step codeine 3rd NSAIDS intermittently Intra-articular corticosteroid injection produces short term improvement when there’s painful joint effusion Most medications are unproven; bisphosphonates and tissue metalloproteinases or cytokines Sx: Surgery Joint replacements Realignment Excision athroplasty |
Describe the role of aids and adaptations in the management of joint disease.
Different aids and devices can be used in the management of OA to take the stress of painful joints and alleviate painful symptoms.
- Healthcare professionals should offer advice on appropriate footwear (including shock-absorbing properties) as part of core treatment for people with lower limb osteoarthritis.
- People with osteoarthritis who have biomechanical joint pain or instability should be considered for assessment for bracing/joint supports/insoles as an adjunct to their core treatment.
- Assistive devices (for example, walking sticks and tap turners) should be considered as adjuncts to core treatment for people with osteoarthritis who have specific problems with activities of daily living. Healthcare professionals may need to seek expert advice in this context (for example, from occupational therapists or Disability Equipment Assessment Centres).
- Healthcare professionals should offer advice on appropriate footwear (including shock-absorbing properties) as part of core treatment for people with lower limb osteoarthritis.
- People with osteoarthritis who have biomechanical joint pain or instability should be considered for assessment for bracing/joint supports/insoles as an adjunct to their core treatment.
- Assistive devices (for example, walking sticks and tap turners) should be considered as adjuncts to core treatment for people with osteoarthritis who have specific problems with activities of daily living. Healthcare professionals may need to seek expert advice in this context (for example, from occupational therapists or Disability Equipment Assessment Centres).
Describe the role of the Physiotherapist and Occupational Therapist in the management of joint disease.
Physiotherapist:
Management Role –
Pain relief –
· Heat Therapy, Cryotherapy, Paraffin Wax therapy
· Manual Therapy – Carpal Bone Mobilisation for short term pain relief
Structural Devices:
· Hand Splinting – short term relief of Carpal Tunnel Syndrome
· Foot Orthotics/Prescriptioned Footwear – decreased pain in RA on weightbearing activity.
Exercise:
· Slows down loss of bone mineral density – discourages use of high impact loading activity in RA patients with severe structural damage
· Maintaining Range of Movement (ROM) – exercise facilitates tendon gliding which improves cartilage nutrition and max. available range of motion
· Maintaining Strength
Long Term Management:
Self Management –
· education and coping strategies – incorporating exercise regimes with exercise to reduce pain and increase function
Role of OT:
· To Promote independence through modification of the performance, task and technique/environment
Services: Care of elderly, early intervention, primary care teams, Hospice, Disability, Psychiatric, Intellectual Disabilities, Seating
OT Assessment of Case –
· Role in early referral.
· Staging – Acute, Subacute, chronic-active, chronic inactive
· ROM, Strength, hand function, sensation, endurance, performance, goals, motivation
· Activities of Daily Living (ADL)
· Functional Transfers
· Leisure and Hobbies
· Home/Work Environment
· Task Analysis
Treatment Objectives:
Maintain/increase joint mobility, maintain increase muscle strength, increase physical endurance, prevent or correct deformities, minimise effect of deformities, maintain independence, knowledge of disease and strategies, stress management
Intervention:
· Joint protection, energy conservation respect pain, task simplification/modification, modify environment, adaptive environment, psychological impact, Home programme
· Splinting: Resting splints, functional stabilising splints, dynamic splints (correct positioning), Progressive splinting post surgery (MCP joint replacement arthroplasty)
· Support and Understanding!
Management Role –
Pain relief –
· Heat Therapy, Cryotherapy, Paraffin Wax therapy
· Manual Therapy – Carpal Bone Mobilisation for short term pain relief
Structural Devices:
· Hand Splinting – short term relief of Carpal Tunnel Syndrome
· Foot Orthotics/Prescriptioned Footwear – decreased pain in RA on weightbearing activity.
Exercise:
· Slows down loss of bone mineral density – discourages use of high impact loading activity in RA patients with severe structural damage
· Maintaining Range of Movement (ROM) – exercise facilitates tendon gliding which improves cartilage nutrition and max. available range of motion
· Maintaining Strength
Long Term Management:
Self Management –
· education and coping strategies – incorporating exercise regimes with exercise to reduce pain and increase function
Role of OT:
· To Promote independence through modification of the performance, task and technique/environment
Services: Care of elderly, early intervention, primary care teams, Hospice, Disability, Psychiatric, Intellectual Disabilities, Seating
OT Assessment of Case –
· Role in early referral.
· Staging – Acute, Subacute, chronic-active, chronic inactive
· ROM, Strength, hand function, sensation, endurance, performance, goals, motivation
· Activities of Daily Living (ADL)
· Functional Transfers
· Leisure and Hobbies
· Home/Work Environment
· Task Analysis
Treatment Objectives:
Maintain/increase joint mobility, maintain increase muscle strength, increase physical endurance, prevent or correct deformities, minimise effect of deformities, maintain independence, knowledge of disease and strategies, stress management
Intervention:
· Joint protection, energy conservation respect pain, task simplification/modification, modify environment, adaptive environment, psychological impact, Home programme
· Splinting: Resting splints, functional stabilising splints, dynamic splints (correct positioning), Progressive splinting post surgery (MCP joint replacement arthroplasty)
· Support and Understanding!
