Case Summary
Describe the process of inflammation, healing and repair in relation to soft tissue trauma
Review the process of inflammation and healing and repair in relation to soft tissue trauma
- Bleeding phase
- Following soft tissue injury, blood will escape into the tissues. Muscles will bleed more than ligaments.
- Clotting cascade to stop blood loss
- Inflammatory phase
- Initial quick vasoconstriction to stop blood loss followed by vasodilation and increased permeability due to histamine, prostaglandins and bradykinin released by local cells
- Heat, redness, pain, swelling, loss of function
- Activated local macrophages produce TNF, IL-1, IL-6 which recruit leukocytes
- These cytokines induce endothelial cells to express adhesion molecules for leuckocyte margination and adhesion.
- First cells in are neutrophils, then come macrophages
- Inflammatory cells come in and remove damaged tissue and debris and recruit growth factors and fibroblasts to injury site to get ready for healing
- These cytokines induce endothelial cells to express adhesion molecules for leuckocyte margination and adhesion.
- Initial quick vasoconstriction to stop blood loss followed by vasodilation and increased permeability due to histamine, prostaglandins and bradykinin released by local cells
- Proliferation phase (3 -21 days)
- Fibroblasts create granulation tissue – first layer of wound repair
- Angiogenesis – because activity of fibroblasts require oxygen and nutrients, angiogenesis builds new blood vessels to area of wound
- Fibroblasts then synthesize scar tissue (type III collagen) to repair.
- Remodeling (21 days to months, years)
- Cross linking and shortening of collagen fibers to promote tight strong scar
- Remodeling of collagen to increase functionality, and type III collagen replaced by stronger type I collagen.
- Scar not as strong as normal tissue. Goal is for scar to gain strength and stability.
NSAIDs musculoskeletal injuries |
Midazolam anesthesia |
|
NSAIDS inhibit COX which catalyses the synthesis of prostaglandins and thromboxane from arachadonic acid
There are 2 isoforms of COX COX 1 o Constantly expressed in most cells o Maintenance role in tissue homeostasis COX 2 o Induced when inflammatory cells are activated (mostly activated by IL1 and TNF alpha) o Produces the prostaglandin mediators of inflammation, thus reducing it As a rule of thumb Anti-inflammatory = COX2 Adverse effects eg GI – loss og PGI2 and PGE2 = COX 1 Cox 2 SELECTIVE drugs are 5 times more potent than non COX 2 Selective drugs Uses - Analgesia - Anti-inflammatory - Antipyretic - Anti platelet Controversy - Inflammation is part of the healing process - Decrease inflammation may prove counterproductive - Some literature suggests NSAIDS may delay rate of fibre regeneration and make cause long term damage - Still a strong analgesic so is widely used - No studies have yet proved conclusive |
Midazolam is a short acting hypnotic-sedative drug of the BZD class. It has powerful anxiolytic properties and is used as an anesthetic preparation (IM/IV 1-5mg) in order to produce anteriograde amnesia of surgery performed.
General Benzodiazepine MOA
Nausea, Dizziness, Vomiting, Prolonged Amnesia, Ataxia, Slurred Speech Heavy interaction with other psychoactive agents Renal excretion |
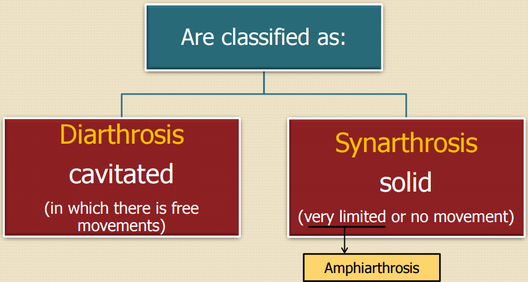
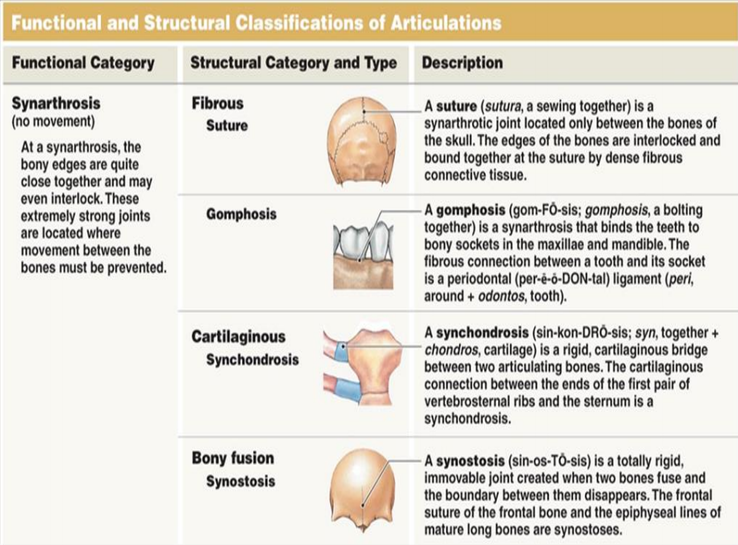
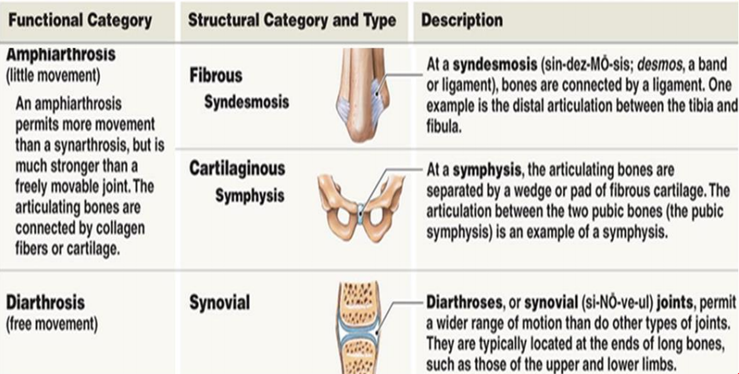
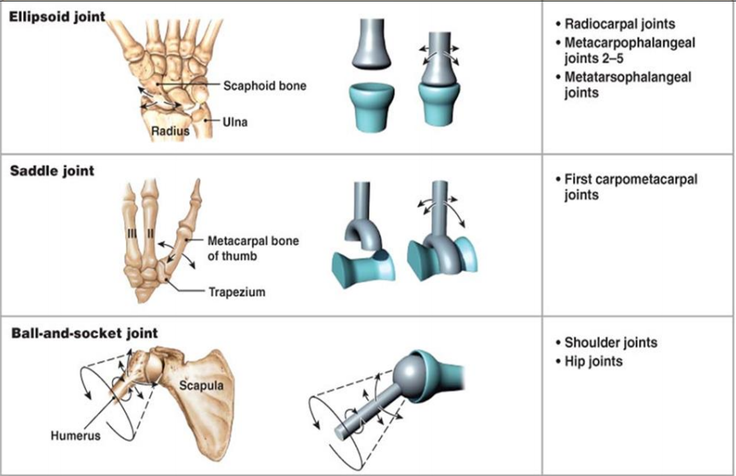
Describe and classify joints
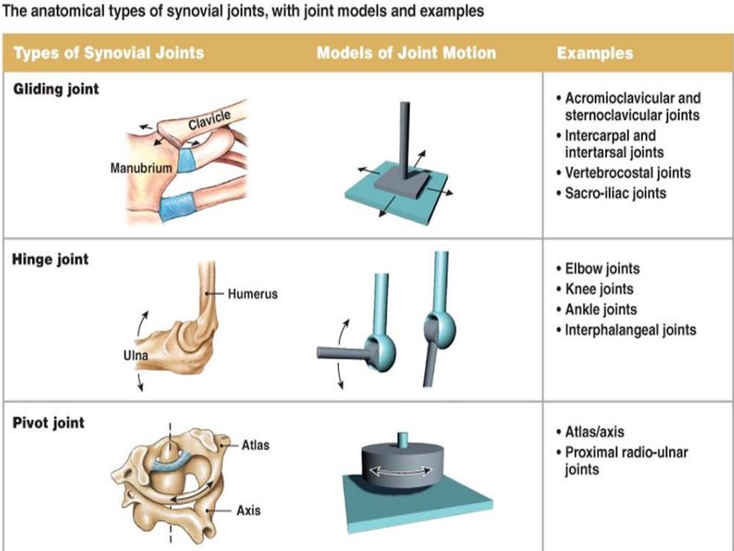
Describe the joints of the shoulder complex and the three articulations of the elbow
|
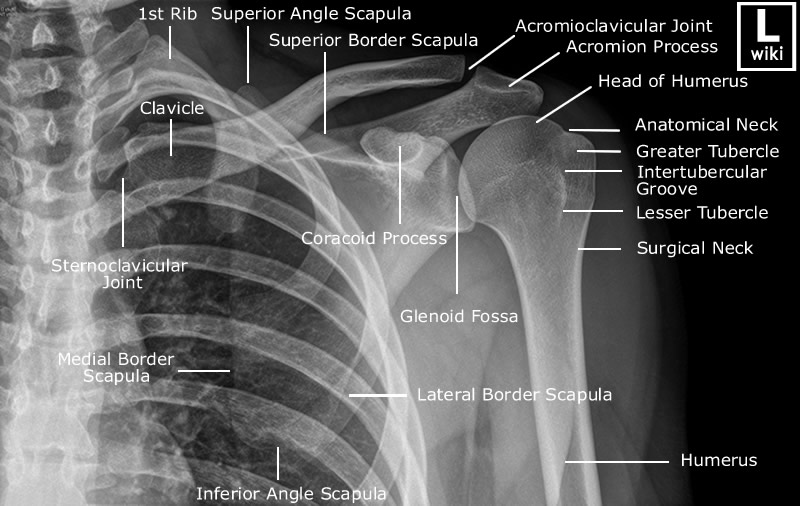
The Three Joints Shoulder Joints
|
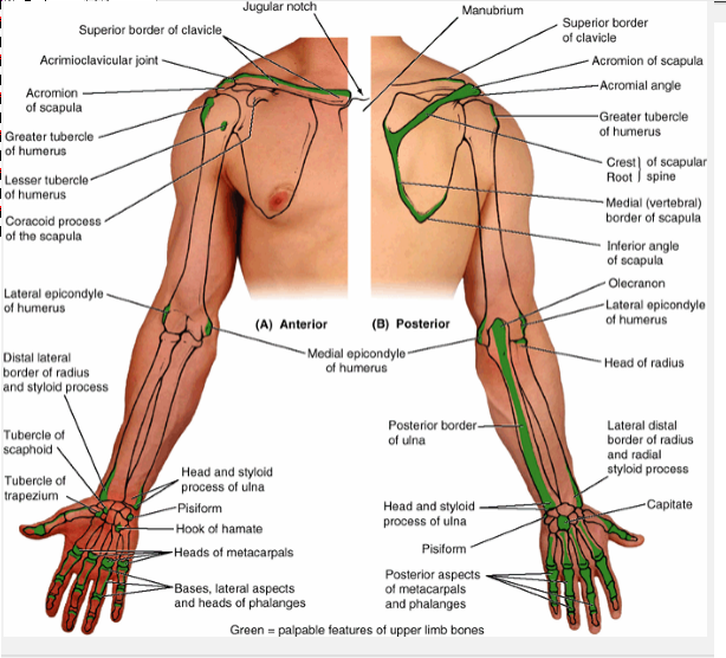
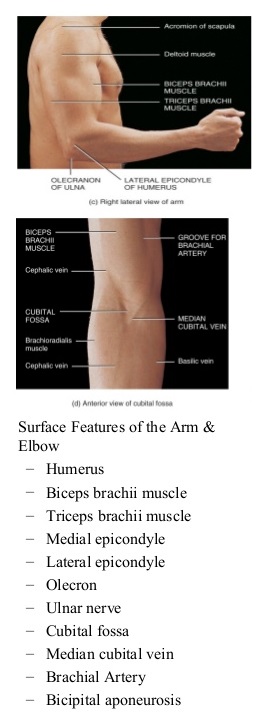
Surface position of bony landmarks of the shoulder girdle and elbow
|
|
|
Explain the movements available in the shoulder complex and the elbow and relate the movements to the joint structure
|
|
Identify the ligaments associated with these joints and their functional significance in terms of mobility and stability
Acromioclavicular joint
Is a plane type synovial joint between the lateral end of the clavicle and the acromion of the scapula.
Outer fibrous layer of the joint capsule is thickened to form 5 intrinsic ligaments that support the joint.
III. Subclavius – anchors and depresses clavicle
IV. Serratus anterior – protracts and rotates scapula and holds it against thoracic wall = punching muscle
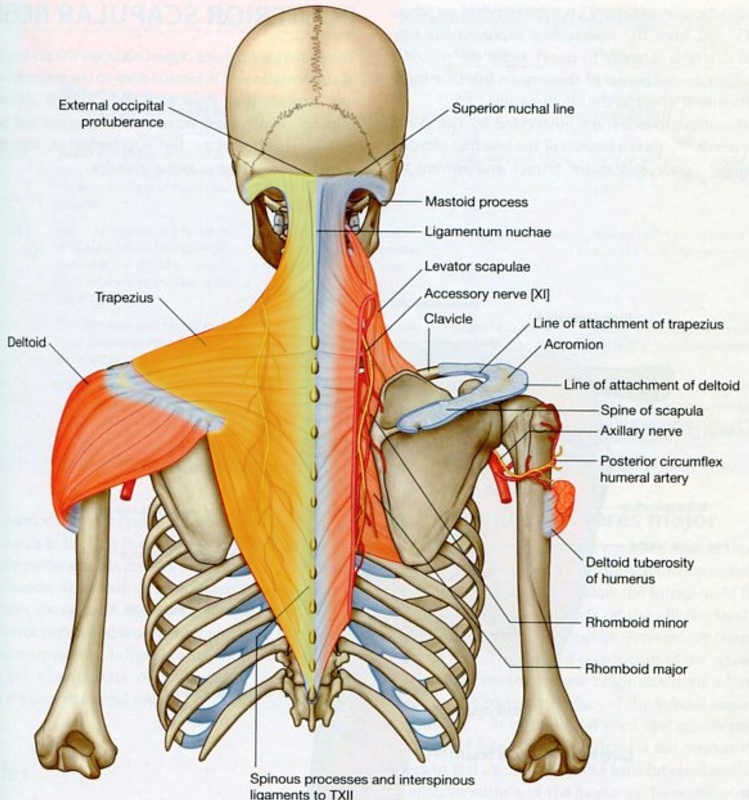
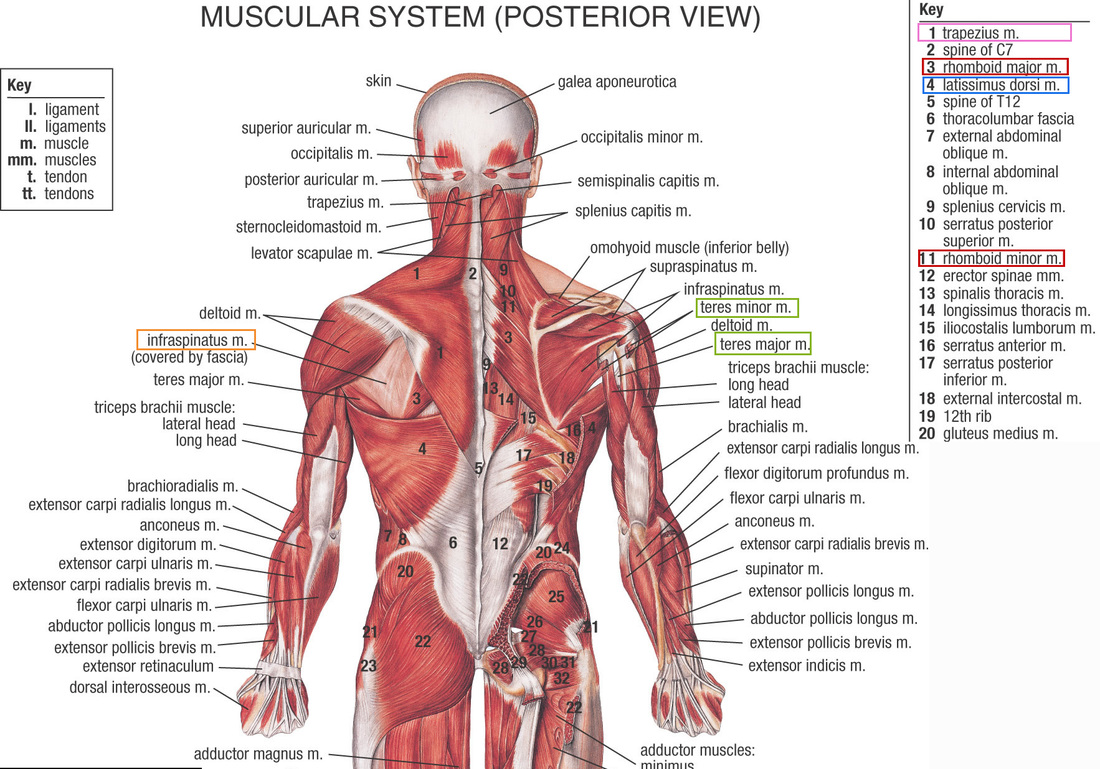
Three groups of posterior shoulder muscles
1. Superficial posterior (extrinsic)
Deltoid (C5, 6)
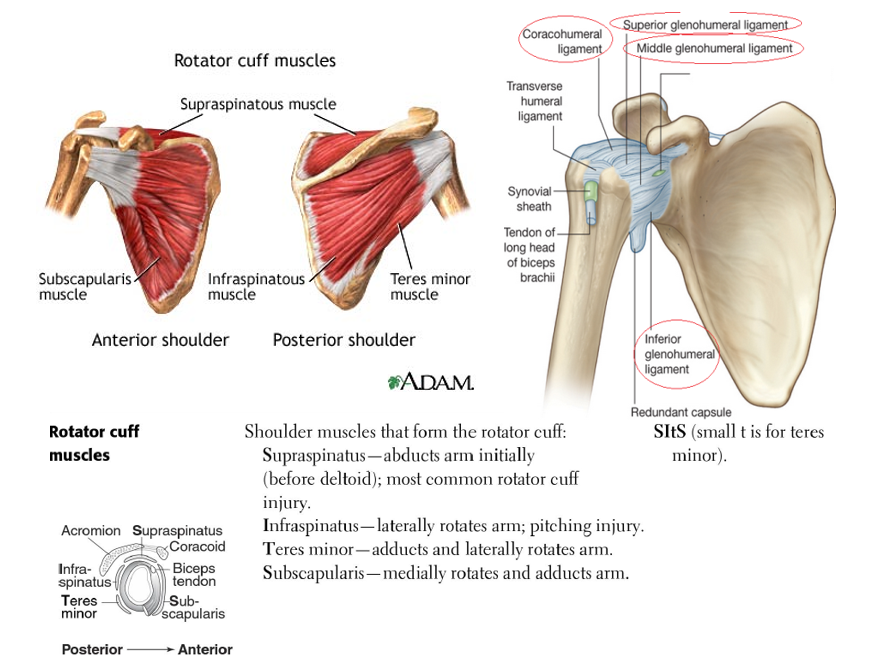
Rotator cuff muscles – these originate on the scapula and blend with and reinforce fibrous layer of the joint capsule in all directions but inferiorly
Supraspinatus (C4, 5, 6) – superior facet greater tubercle
Blood supply - Anterior and posterior circumflex humeral arteries and branches of suprascapular artery
Is a plane type synovial joint between the lateral end of the clavicle and the acromion of the scapula.
- Ligaments
- Acromioclavicular ligament – extends from the acromion to the clavicle strengthening the joint superiorly
- Coracoclavicular ligaments – extend from coracoid process of scapula to the clavicle, anchoring the clavicle to the coracoid process.
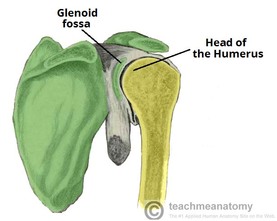
- Ball and socket type of synovial joint
- The large round humeral head articulates with the shallow glenoid cavity of the scapula, which accepts 1/3 of the humeral head.
- Ring like glenoid labrum outlines the glenoid cavity and slightly deepens the cavity.
- Tendon of long head of biceps is continuous with glenoid labrum
- The joint capsule surrounds the joint and attaches medially to the glenoid cavity and laterally to the anatomical neck of the humerus.
Outer fibrous layer of the joint capsule is thickened to form 5 intrinsic ligaments that support the joint.
- 3 Glenohumoral ligaments
- Three (sup, middle, inf) fibrous bands that reinforce anterior part of joint capsule.
- Coracohumeral ligament
- From coracoid to greater tubercle, supports joint superiorly
- Transverse humeral ligament
- Runs from the greater to the lesser tubercle of the humerus. Holds the synovial sheath and tendon of biceps brachi in place during movement of shoulder.
- Coraco-acromial arch
- Ligament that spans from acromion and to coracoid process of the scapula, forming a protective arch over the humeral head to prevent superior displacement.
- Four anterior muscles move the pectoral girdle
- Has two heads, clavicular and sternocostal
- When acting together, adduction, medial rotation; independently the clavicular head causes flexion and sternocostal causes extension
III. Subclavius – anchors and depresses clavicle
IV. Serratus anterior – protracts and rotates scapula and holds it against thoracic wall = punching muscle
Three groups of posterior shoulder muscles
1. Superficial posterior (extrinsic)
- Trapezius (motor XI spinal accessory, sensory from C3, C4) – attaches the pectoral girdle to cranium and vertebral column
- Latissimus dorsi (C6, 7, 8) – raises body when climbing
- Levator scapula
- Rhomboids
Deltoid (C5, 6)
- Clavicular (ant) part – flexes and medially rotates arm
- Acromial (middle) part – abducts arm
- Spinal part (post) – extends and laterally rotates arm
Rotator cuff muscles – these originate on the scapula and blend with and reinforce fibrous layer of the joint capsule in all directions but inferiorly
Supraspinatus (C4, 5, 6) – superior facet greater tubercle
- Initiates and assists deltoid with first 15 degrees of abduction
- Laterally rotates arm
- Laterally rotates arm
- Medially rotates arm
Blood supply - Anterior and posterior circumflex humeral arteries and branches of suprascapular artery
Anatomy of elbow joint
Elbow joint
Radial collateral ligament
Elbow joint
- Hinge type synovial joint, located 2 cm inferior of epicondyles of humerus
- The trochlea of the humerus articulates with the trochlear notch of the ulna, and the capitulum of the humerus articulates with the concave head of the radius. And the radius articulates with the ulna at the proximal radio-ulnar joint, which is a pivot synovial joint.
Radial collateral ligament
- On lateral side, extends from lateral epicondyle of the humerus and blends distally with the anular ligament of the radius.
- On medial side, 3 bands extend from the medial epicondyle of the humerus to the coronoid process and olecranon of the ulna
- Holds the head of the radius in the radial notch of the ulna to form the proximal radio-ulnar joint.
Describe the general principles affecting stability and mobility of joints
Shape, Size and Arrangement of Articular SurfacesThe joints of the body come in all shapes and sizes. The most important factor to consider here is the relative proportion of the two articulating surfaces.
For example, in the shoulder joint, the humeral head of the upper arm is disproportionately larger than the glenoid fossa of the scapula that it sits into – making the joint more unstable, as there is less contact between the bones.
In contrast, the acetabulum of the pelvis fully encompasses the femoral head, and this makes the hip joint far more stable. However, while the hip is more stable, the shoulder has a greater range of movement. Each joint has this trade off that is particular to its function.
For example, in the shoulder joint, the humeral head of the upper arm is disproportionately larger than the glenoid fossa of the scapula that it sits into – making the joint more unstable, as there is less contact between the bones.
In contrast, the acetabulum of the pelvis fully encompasses the femoral head, and this makes the hip joint far more stable. However, while the hip is more stable, the shoulder has a greater range of movement. Each joint has this trade off that is particular to its function.
|
Ligaments
|
Tone of Surrounding Muscles
- The tone of the surrounding muscles contributes greatly to the stability of a joint. An good example of this are the rotator cuff muscles, which keep the head of the humerus in the shallow glenoid cavity of the scapula. If there is a loss of tone, such as in old age or stroke, the shoulder can dislocate.
- Dislocations of the shoulder joint can tear the rotator cuff muscles, making the patient more susceptible to further injuries.
- Similarly, the tone of muscles around the knee are crucial to its stability. Through inappropriate or unbalanced training, the knee can be made prone to injury through muscle imbalance. This can lead to chronic pain.
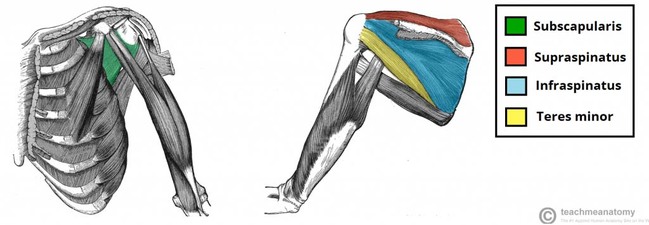
[ S I T S ]
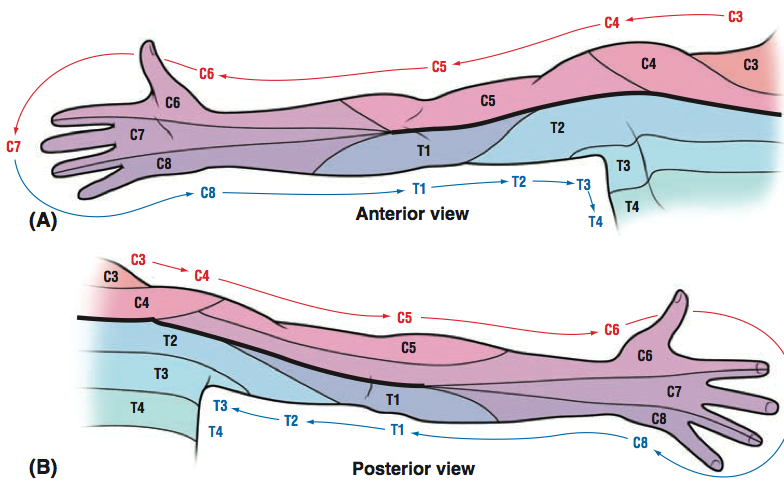
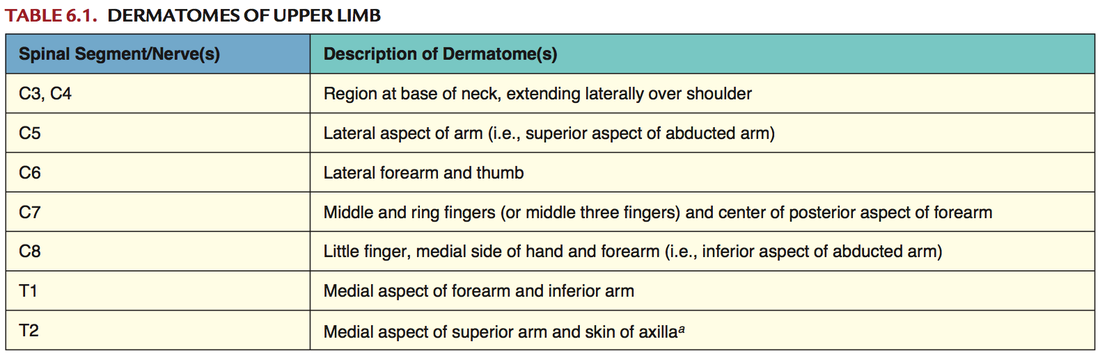
Describe in general terms the functional consequences of minor nerve injury
Describe in general terms functional consequences of minor nerve injury
- Consequences of nerve injury depend on the extent of the injury, whether the nerve is in PNS or CNS, and the age of the person.
- When an axon is damaged, the distal segment undergoes Wallerian degeneration, losing its myelin sheath, while the proximal segment either dies or attempts to repair.
- The PNS is able to repair and regenerate.
- Following nerve damage, phagocytes clear debris and damaged tissue, and then schwann cells oversee that the proximal end sprout axon and is directed to grow back to correct target.
- The CNS, for the most part, is not capable of repair.
- Glial cells quickly form scars following nerve damage
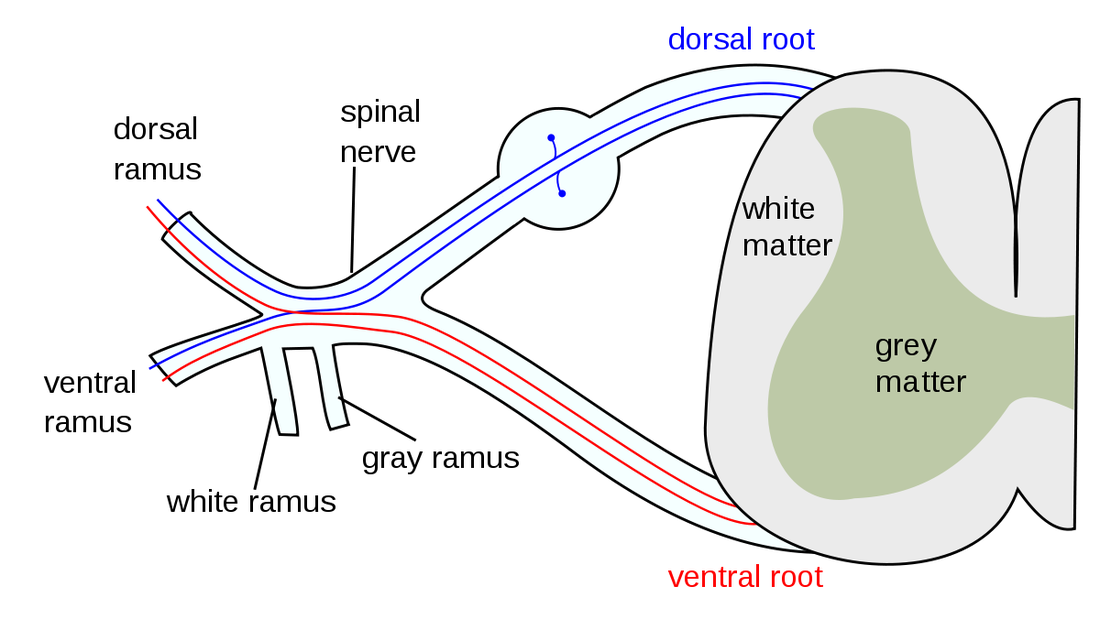
- Each nerve is wrapped in a protective sheath called the endoneurium. The nerves are bundled together in fascicles and surrounded by the perineurium. Several fascicles are bundled together within the epineurium.
- The worse the damage, the less likely repair is possible.
- Types of damage
- Neurapraxia
- Least severe form of nerve injury
- Compression of the nerve or disruption in blood supply (ischemia) causes an interruption in the conduction of the impulse down the nerve fiber. Results in temporary loss of function which is reversible.
- Axonotmesis
- Axon and myelin sheath are damaged, but endoneurium, perineurium, and epineurium are intact.
- Can cause paralysis of motor, sensory, and autonomic activity.
- Mainly seen in crush injuries.
- The axon may regenerate
- Worse versions of axonotmesis where there is damage to endoneurium
- Neurotmesis
- Severe injury in which the nerve is damaged to the point where the axon, myelin, and endoneurium, perineurium and epineurium are damaged
- Neurapraxia
Explain the effect on joint mobility and functional consequences to an individual following
a) Glenohumeral dislocation
Shoulder dislocation (what it is, anterior vs posterior, causes, how to treat and long term complications)
- Because of its freedom of movement and instability, glenohumeral joint is commonly dislocated.
- Coraco-acromial arch and rotator cuff muscles are effective at preventing upward dislocation, so most dislocations are downwards (inferior), however, they are described clinically as anterior or rarely posterior, depending on whether humeral head has descended anterior or posterior to the infraglenoid tubercle (inferior edge of glenoid cavity where triceps originate)
- Most common
- Usually caused by falling on an outstretched arm – arm is abducted, extended, and externally rotated, a hard blow will tilt head of humerus inferiorly to the weak part of the joint capsule (stretching or tearing the labrum or ligaments). Subsequently, the strong flexor and adductor muscles usually pull the humeral head anterosuperiorly into a subcoracoid position.
- Arm is internally rotated and adducted
- Due to electric shock or seizure
- Treatment
- Externally rotate slowly, or massage muscles, or pull on it like crazy
- X-ray to make sure reduction successful
- Arm should be immobilized in a sling for several days (in external rotation)
- In some cases, may need surgery to repair damage to tissues surrounding shoulder joint
- Rotator cuff strengthening exercises
- Axillary nerve damage
- Resulting in paralyzed deltoid. Deltoid will atrophy, rounded shoulder lost, and patient will have difficulty abducting arm past 15 degrees
- Damage to brachial plexus
- Axillary artery damage
- Hematoma, peripheral cyanosis, coolness, pulse deficit
- Rotator cuff tear
- Hill-Sachs fracture
- Is a depression in the posterolateral head of the humerus from the impact of the humeral head against the anteroinferior glenoid rim when the shoulder is dislocated anteriorly
- Can contribute to future shoulder instability
- Long term complications
- Recurrent shoulder dislocations
- Bankart lesion
- Is an injury to the anterior glenoid labrum from repeated anterior dislocation
- A bony bankart includes a fracture of the anterior inferior glenoid cavity
b) Nerve injury
|
|
Relate nerves at risk from dislocation to the glenohumeral joint, the humerus and muscles of the arm and the elbow joint
Common nerve injuries in the upper limb. Nerves at risk from dislocations and injuries to arm

|
Erb-Duchenne Palsy
Injury to superior trunk (C5, C6) Loss of the upper trunk (C5-C6) due to seat belt Result: Adducted and medially rotated arm, extended elbow with flexed wrist
|
Why Adducted?
- C5-C6 à upper trunk à lateral cord à musculocutaneus nerve (MC)
- MC supplies the deltoid and the supraspinatus (both abductors)
- Abduction is lost so the arm is adducted
- The main lateral rotators are infraspinatus, teres minor and the posterior deltoid (C5-C6) whereas the medial rotators include pectoralis major and latissimus dorsi.
- Lateral rotation is lost so the arm is medially rotated
- The elbow flexor compartment is all C5-C6 (biceps, brachioradialis and brachialis) so flexion is lost and the elbow is extended
- The biceps is the main supinator (in a flexed position) and that is lost so the forearm is pronated
- Extensor Carpi radialis longus, despite innervation from the radial nerve, is C5-C6 and that is lost so the wrist is flexed
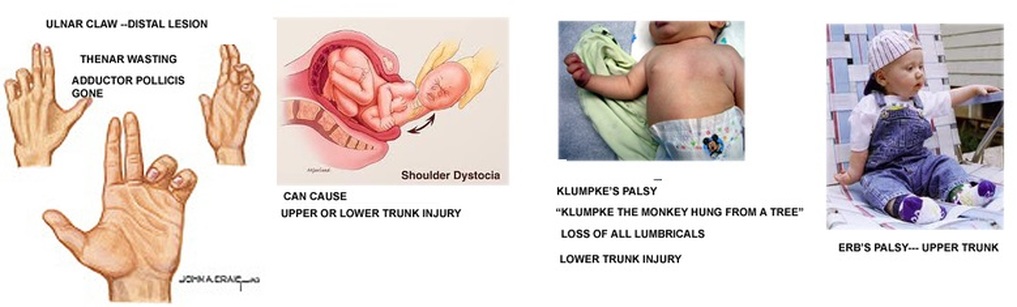
Klumpke’s Palsy
- Damage to inferior trunk (C8, T1)
- This completely takes out ulnar nerve and some of median nerve. The part of the median nerve that is affected is it’s most distal innervations.
- The result is a complete loss of all lumbricals, and unopposed action of finger flexors (median nerve) and finger extensors (radial nerve), which flex the IP and extend the MCP respectively giving the appearance of a total claw hand (flexors stronger then extensors in the IP, but extensors unopposed in MCP).
- Often also see horner’s syndrome


|
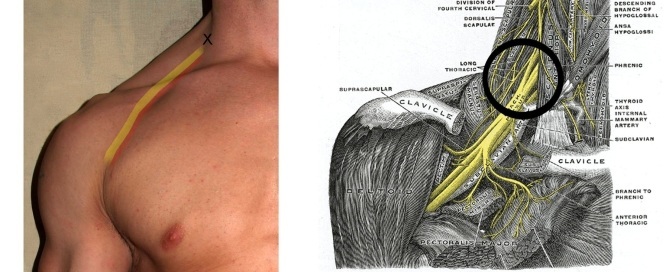
Winged Scapula don't forget this! its an easy mark = long thoracic nerve
|
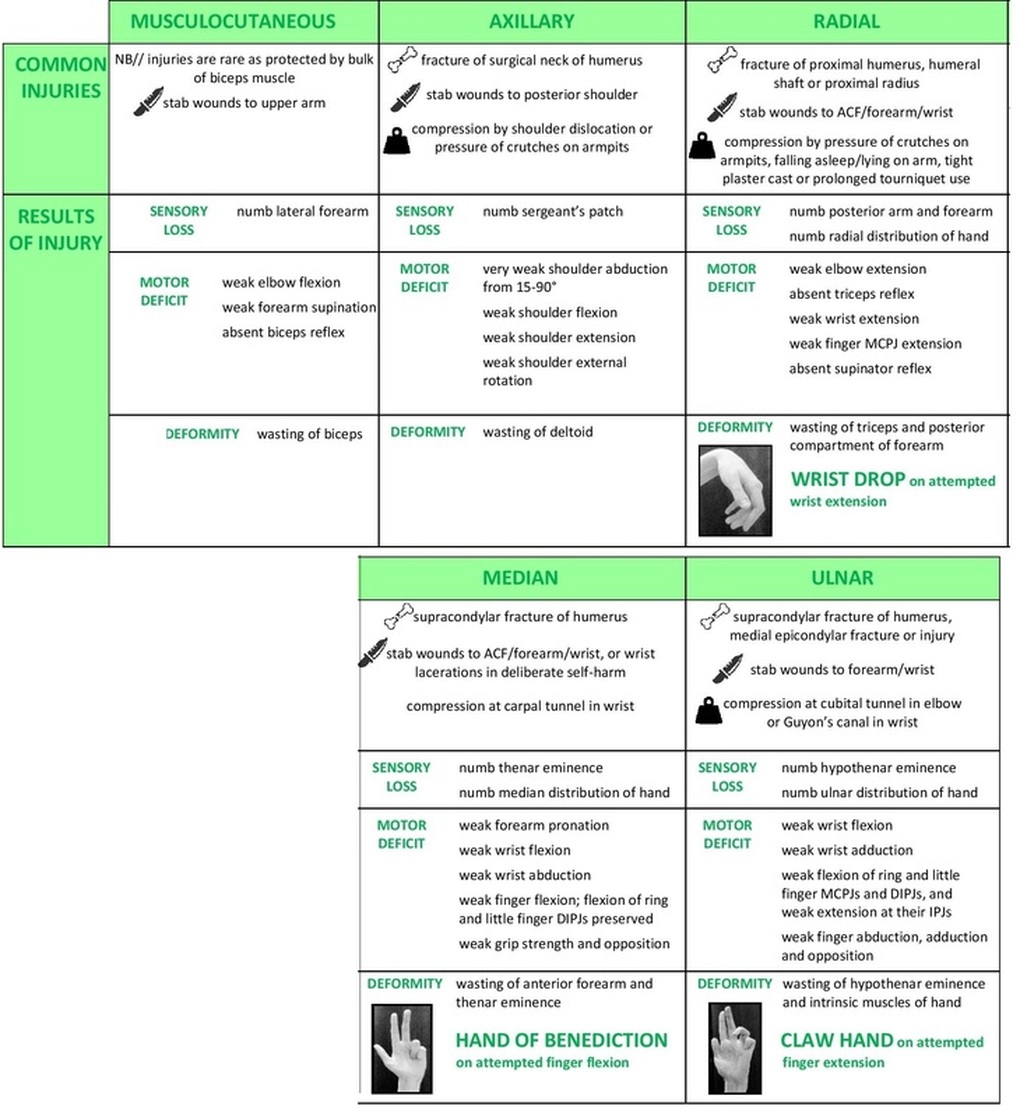
Injury to axillary nerve (C5, C6)
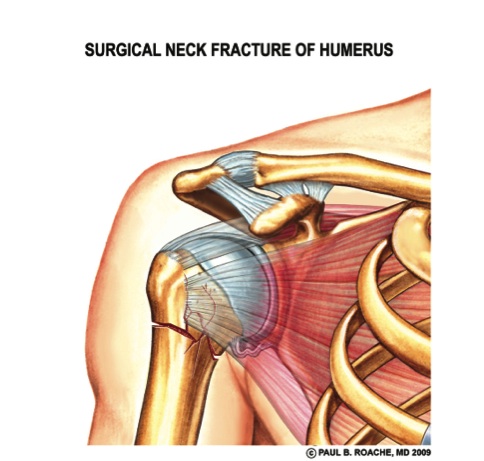
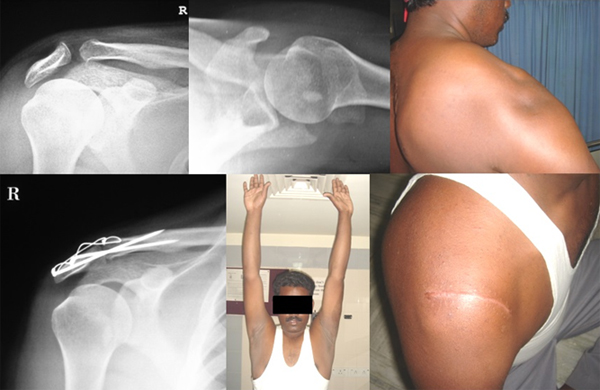
- Caused by fracture of surgical neck of humerus or anterior dislocation of humeral head
- Motor deficit to deltoid and teres minor so patient can’t abduct arm at shoulder and sensory deficit over deltoid muscle (atrophy of deltoids).
- Fracture to mid shaft of humerus can damage radial nerve in the radial groove
- Has already given off branches to triceps, so elbow can be extended, but muscles of extension in the posterior compartment of the arm are paralyzed, so there is wrist drop due to unopposed flexion of wrist and fingers. Also weak supination because supinator gone.
- Also sensory deficit to posterior forearm and dorsum of hand and lateral 3.5 fingers
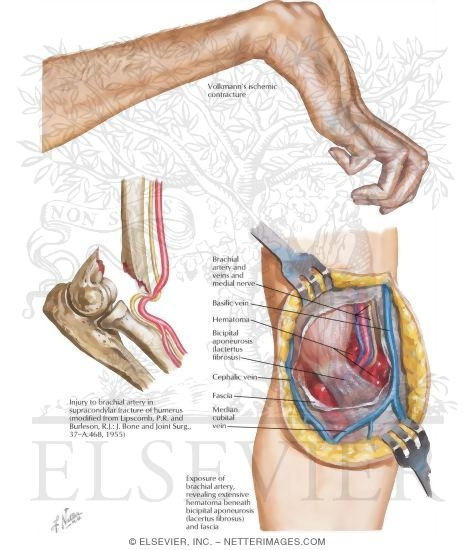
- Fracture of distal humerus just before epicondyles (supraepicondyle)
- Damages median nerve, paralyzing flexors and pronators in the forearm with the exception of flexor carpi ulnaris and medial half of flexor digitorum profundus. Forearm will constantly be supinated, and flexion will be accompanied by adduction. No flexion of thumb (atrophied), and 1st and 2nd lumbricals paralyzed, so patient cannot flex MCP or extend IP of 2nd and 3rd finger.
- Hand of benedict when patient tries to make a fist, as 4th and 5th fingers can flex, but others cannot.
- Ulnar innervates:
- Hypothenar muscles, 3rd and 4th lumbricals, dorsal and palmar interossei, adductor pollicis, medial half of flexor digitorum profundus, and flexor carpi ulnaris
- If she tries to flex her wrist, it will also abduct because it is being flexed solely by flexor carpi radialis, which also abducts wrist.
- MCP of 4th and 5th fingers will be extended because of loss of 3rd and 4th lumbricals, but neither flexion or extension at IP because of loss of lumbricals and medial flexor digitorum profundus
- Sensory deficit to palmar and dorsal medial 1 and a half fingers
|
Volkmann’s Ischemic Contracture
|
|
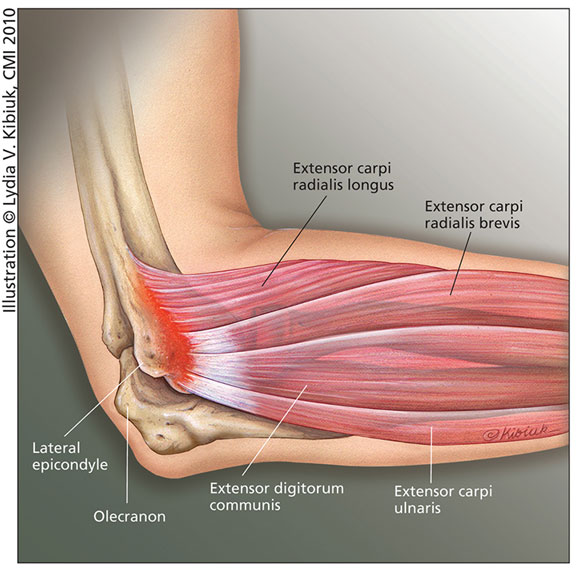
Tennis Elbow (Epicondylitis)
Fracture of surgical neck of humerus
|
|
Short and long term complications that arise from a dislocated shoulder

|
Dislocated Glenohumeral Joint
Intrinsic Ligaments – Resist Anterior Dislocation
|
Rotator Cuff Muscles – Resist most other dislocation
|
|
Acromion Fracture
|
|
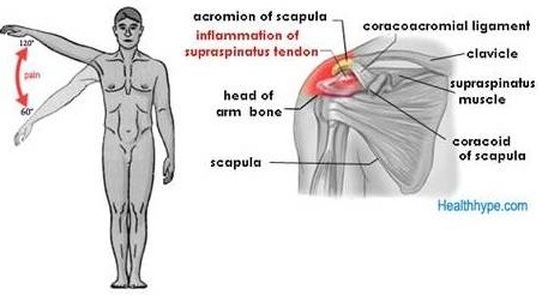
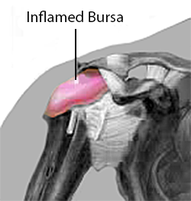
Supraspinatus Tendonitis + Bursitis
- The supraspinatus initiates abduction. Note that the deltoid cannot initiate abduction because when the arm is fully adducted the angle means that the deltoid can only lift the humerus. Once abduction has been initiated by the supraspinatus (15 degrees) the deltoid does most of the work.
- Know the route of the supraspinatus from the suprascapular fossa à under the corico-acromial ligament à greater tubercle
- Between the tendon of the supraspinatus and the ligament is a fluid filled sac called the subacromial bursa
- This reduces tension between the supraspinatus ligament, acromion and the corico-acromial ligament.
- If the sac becomes inflamed pain will be felt all the way to the hand on abduction
- Calcium may also deposit in the supraspinatus tendon causing increased pressure and pain but also may even rupture the deltoid tendon
- Workaround:
- Loss of the action of the supraspinatus cannot be made up for with the deltoid in full adduction but if the patient tilts their body laterally and let their arm hang there will be enough angle for the deltoid to abduct.
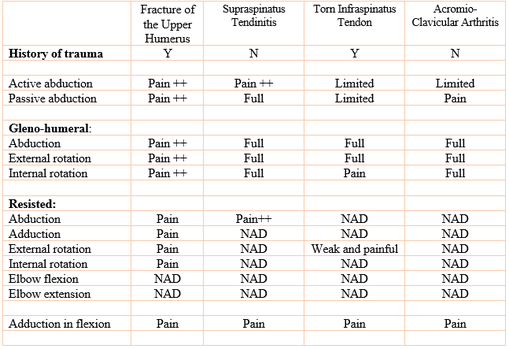
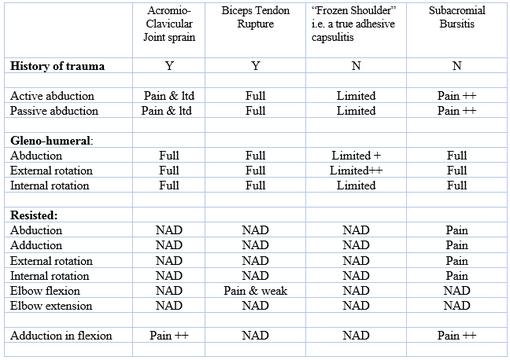
- Tests (see clinical skills doc):
- Difficulty with the arm drop test = rotator cuff tear; Painful ark on abduction; Coke can emptying test
|
|
Describe the anatomical and physical basis of treatment options for shoulder and elbow problems ranging from conservative management to surgical intervention
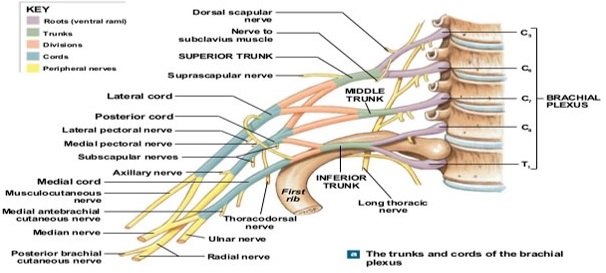
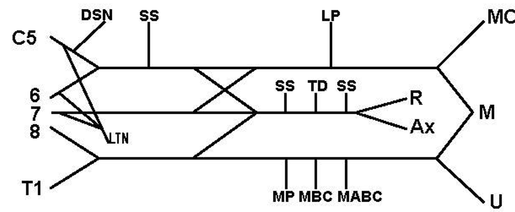
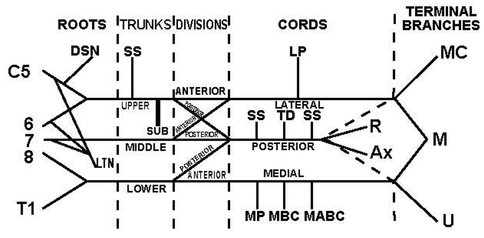
Describe the relationship of the components of the brachial plexus to the glenohumeral joint
The brachial plexus is a network of nerves, running from the spine, formed by the anterior rami of the lower four cervical nerves and first thoracic nerve(C5–C8, T1). The brachial plexus passes through the cervicoaxillary canal in the neck, over the first rib, and into the axilla (armpit region), where it innervates the upper limbs and some neck and shoulder muscles.
|
|
|
|
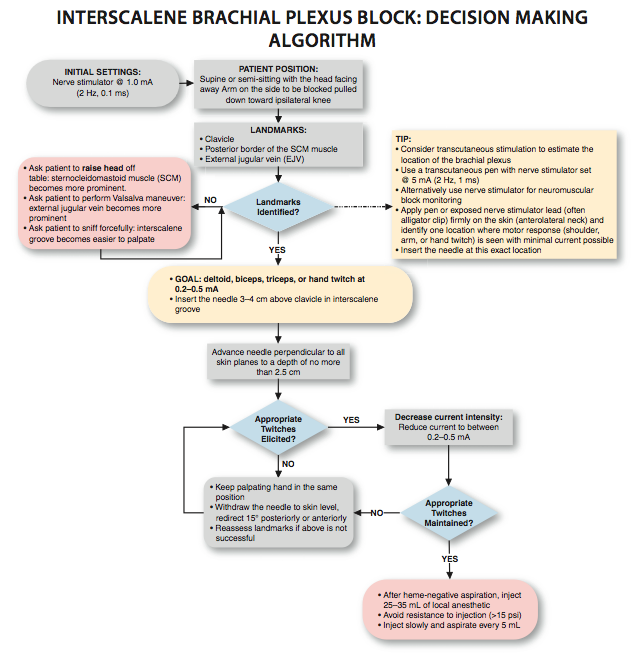
Brachial plexus blocks are regional anesthesia techniques that are sometimes employed as an alternative to general anesthesia for surgery of the shoulder, arm,forearm, wrist and hand.
- These techniques involve the injection of local anesthetic agents in close proximity to the brachial plexus, temporarily blocking the sensation and ability to move the upper extremity.
- The subject can remain awake during the ensuing surgical procedure, or s/he can be sedated or even fully anesthetized if necessary.
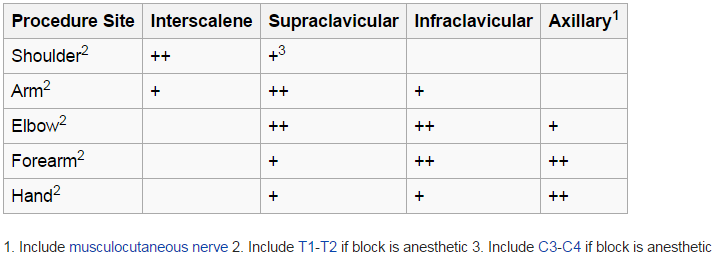
Indicated for
Surgery to the clavicle, shoulder or arm
not indicated for forearm surgery - anesthesia is inadequate in the ulnar nerve
Side Effects
Surgery to the clavicle, shoulder or arm
not indicated for forearm surgery - anesthesia is inadequate in the ulnar nerve
Side Effects
- Temporary paresis (impairment of function) of the thoracic diaphragm - as experienced by most individuals
- If local anesthetic ends up blocking the stellate ganglion, the horner's syndrome may ensue in the patient and vocal cord paresis or difficulty swalling as accompanying features
- COPD together with IS Block can cause respiratory failure
- Phrenic nerve paresis on the contralateral side of the neck