Case Summary
Case Summary
Presenting Complaint
Medications Mx - Topical Corticosteroids, Emollients
Allergies
Past Surgical History PSHx
Family History FHx
Mother = Mrs. Jackie Hughes
Baby Sister = Lucy (8 weeks old)
Older Brother = Ben (school)
Father = has atopic dermatitis, can control own dry skin with E45
Social History SHx
Mrs. Hughes appears tired and tense.
Summary
In summary, Sam Hughes is a 3 year old male presenting to the dermatologist with a persistent red, crusty, dry, itchy rash on his face, neck, and flexural sites. His rash is refractory to emollient and topical corticosteroid treatment and further treatment options are being investigated.
Presenting Complaint
- Sam Hughes, 3 year old male, referred to dermatologist to manage a rash present since 3 months of age. Sam’s face and neck appear very red and crusty and has constant sore, red, itchy patches in all flexural sites, neck, and face. In particular he has thick weepy crusting lesions around his ankles, behind his knees, elbows, and neck. His face is red and flaky, with some patches on his trunk. Overall his skin is generally dry and he is constantly trying to rub and scratch his neck and legs.
- Initially his rash affected his face and cradle cap with few patches of red dry skin on his trunk and neck. However, after 18 months the rash has steadily gotten worse.
Medications Mx - Topical Corticosteroids, Emollients
Allergies
Past Surgical History PSHx
Family History FHx
Mother = Mrs. Jackie Hughes
Baby Sister = Lucy (8 weeks old)
Older Brother = Ben (school)
Father = has atopic dermatitis, can control own dry skin with E45
Social History SHx
Mrs. Hughes appears tired and tense.
Summary
In summary, Sam Hughes is a 3 year old male presenting to the dermatologist with a persistent red, crusty, dry, itchy rash on his face, neck, and flexural sites. His rash is refractory to emollient and topical corticosteroid treatment and further treatment options are being investigated.
Describe the normal structure and function of skin.
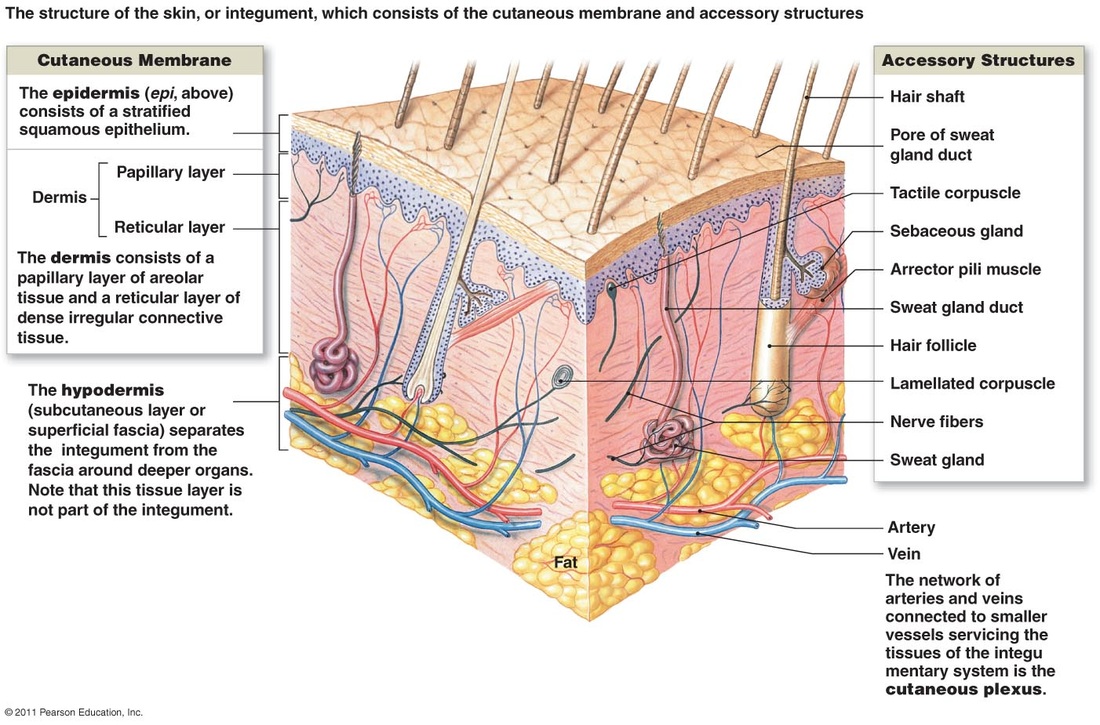
Skin/Integument-Largest organ in the body.
Composed of the Epidermis and Dermis. Underneath the Dermis is a subcutaneous Layer called the Hypodermis/ Superficial Fascia.
Epidermis:
Most superficial layer of skin. Avascular-Receives nutrients from Dermis. Made up of 5 layer but Lucindum is only present in thick skin areas(palm of hands soles of feet).
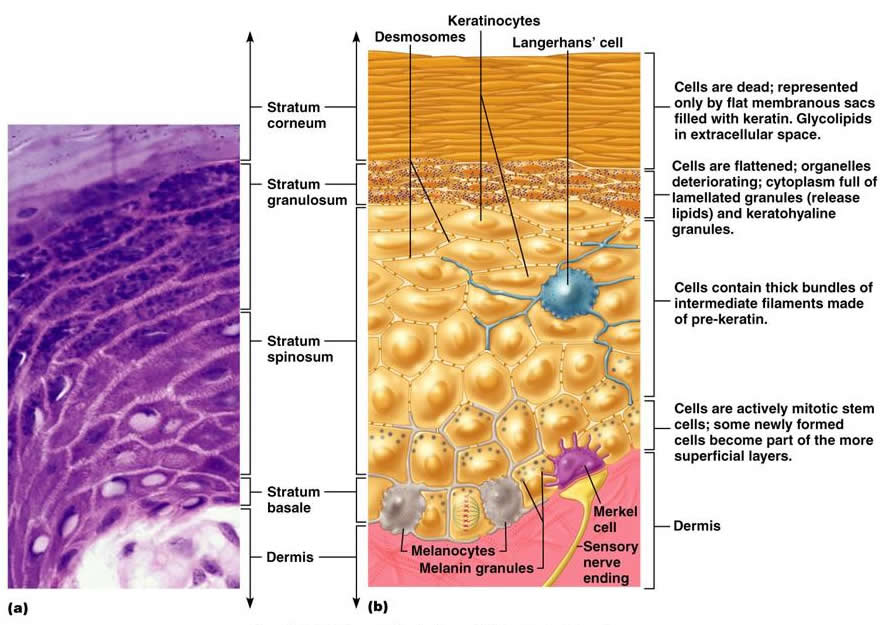
Langerhans cells (readily found in Spinsoum) are APC’s- once antigen is phagocytosed, processed and Displayed on their surface they migrate to a regional lymph node where it interacts with T-Lymphocytes.
Composed of the Epidermis and Dermis. Underneath the Dermis is a subcutaneous Layer called the Hypodermis/ Superficial Fascia.
Epidermis:
Most superficial layer of skin. Avascular-Receives nutrients from Dermis. Made up of 5 layer but Lucindum is only present in thick skin areas(palm of hands soles of feet).
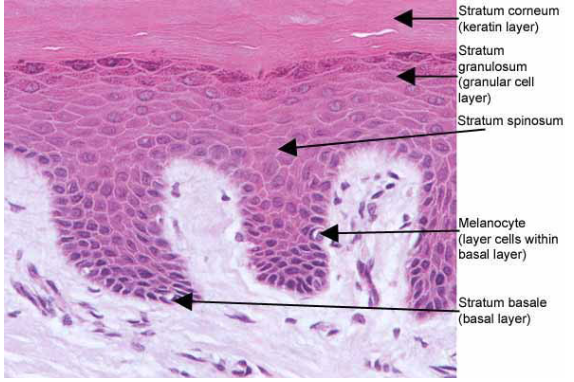
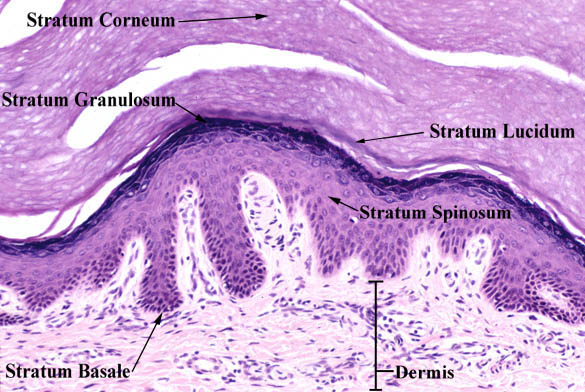
- Stratum Corneum-Anucleate squamous cells with keratin filaments,Thick plasma membrane with extra layer of lipids forming the main Water barrier in the epidermis.
- Stratum Lucidium-considered a subdivision of Corneum. Contains Eosinophilic cells in which keratinisation is well advanced.Progressive loss of nucleus and cytoplasm.
- Stratum Granulosum-Most superficial layer of NON-keratinised cells. Is 1-3 cells thick. Keratinocytes in this layer contain Keratohyalin granules which contain CYS and HIS rich proteins, precursor of Filaggrin responsible for aggregating keratin filaments.
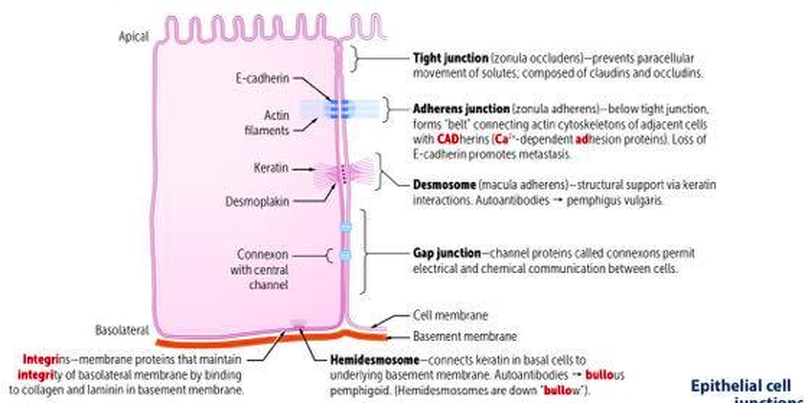
- Stratum Spinosum-Exhibit Spinous processes and is several cells thick. Larger Keratinocytes than in Basale.Processes from one cell are attached to another by Desmosomes. As the cells mature they move to surface and become flattened.
- Stratum Basale –Single layer of cells resting on basal Lamina, cell division occurs here. Contains Stem cells of Keratinocytes. Cells are Small and Cuboidal to low Columnar. 25% of cells in this layer are Melanocytes(derived from neural crest cells)- pigment-producing cells, which are present in the dermo-epidermal junction. Their function is to protect the body from ultraviolet light rays. They produce melanin and secrete into keratinocytes. Melanin is produced from Tyrosine.
Langerhans cells (readily found in Spinsoum) are APC’s- once antigen is phagocytosed, processed and Displayed on their surface they migrate to a regional lymph node where it interacts with T-Lymphocytes.
|
|
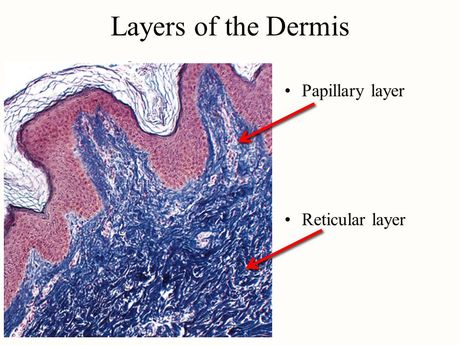
Dermis:
Composed of Papillary Layer and Reticular layer. Contains connective tissue and contains blood and lymph vessels, sensory nerve endings, hair follicles, sweat and sebaceous glands. Other Structures in the Dermis:
● Fibroblasts lie between the collagen bundles and are concerned with collagen and elastin synthesis.
● Macrophages are phagocytic monocytes situated within the tissue.
● Meissner corpuscles are sensory nerves that pick up sensations of touch and relative amounts of pressure.
● Pacinian corpuscles are sensory nerves that pick up sensations of vibration and signal local changes in blood flow.
Papillary Layer- more superficial of two layer of Dermis consists of loose connective tissue. Has delicate collagen meshwork of mainly Type1 and 3 collagen. Elastic fibres also form irregular pattern. Relatively thin and includes the substance of the Dermal Papillae and Dermal Ridges. Contains blood vessels. Contains nerve processes.
Reticular Layer-deep to papillary layer and it thicker and less cellular. Mostly Type 1 collagen and coarse elastic fibres which all form regular lines of tension called Langers lines.
Composed of Papillary Layer and Reticular layer. Contains connective tissue and contains blood and lymph vessels, sensory nerve endings, hair follicles, sweat and sebaceous glands. Other Structures in the Dermis:
● Fibroblasts lie between the collagen bundles and are concerned with collagen and elastin synthesis.
● Macrophages are phagocytic monocytes situated within the tissue.
● Meissner corpuscles are sensory nerves that pick up sensations of touch and relative amounts of pressure.
● Pacinian corpuscles are sensory nerves that pick up sensations of vibration and signal local changes in blood flow.
Papillary Layer- more superficial of two layer of Dermis consists of loose connective tissue. Has delicate collagen meshwork of mainly Type1 and 3 collagen. Elastic fibres also form irregular pattern. Relatively thin and includes the substance of the Dermal Papillae and Dermal Ridges. Contains blood vessels. Contains nerve processes.
Reticular Layer-deep to papillary layer and it thicker and less cellular. Mostly Type 1 collagen and coarse elastic fibres which all form regular lines of tension called Langers lines.
|
Hypodermis:
Supports both the dermis and the epidermis. Also serves as a container for the formation and storage of fat. It contains adipose tissue, connective tissue and supports the blood and lymph vessels and nerve fibres that pass from beneath the tissue into the dermis above. Adipose tissue insulates the body- prevents heat loss and acts as a shock absorber, preventing trauma to underlying structures. It is also a valuable store of triglycerides-a potential source of energy. |
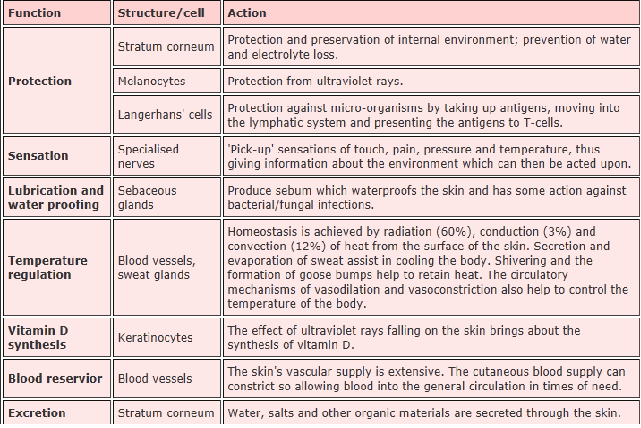
Outline the barrier function of skin.
|
Barrier F(x) of Skin:
|
List the dermatological terms for describing lesions of the skin.

Primary Lesions
Primary lesions are physical changes in the skin considered to be caused directly by the disease process.
Types of primary lesions are rarely specific to a single disease entity.
A. BURROW: burrows are linear/curvilinear lesions produced by infestation of the skin and formation of tunnels (namely by the scabitic mite or by cutaneous larva migrans).
B. COMEDONE: a plug of keratin and sebum wedged in a dilated pilosebaceous orifice
C. MACULE: a circumscribed flat area of altered colour e.g. freckle. A macule greater than 1 cm. may be referred to as a patch.
D. PAPILLOMA: a projecting nipple-like mass e.g. skin tag
E. PAPULE: a discrete elevation of skin that may be changed in colour. Those arising from the subcutis may be felt rather than seen. Larger lesions (>1 cm) are referred to as nodules. Papules may have a variety of shapes in profile (domed, flat-topped, umbilicated) and may be associated with secondary features such as crusts or scales.
F. PETECHIAE and PURPURA: Petechiae are pinhead-sized flat macules of extravascular blood in the dermis.
Purpura are larger and may be palpable
Ecchymosis ('bruise') is where bleeding involves deeper structures
G. PLAQUE: solid, raised, flat-topped area of skin greater than 1cm in diameter. It is analogous to the geological formation, the plateau. e.g. psoriasis plaque
H. PUSTULE: circumscribed elevated lesions that contain pus. They are most commonly infected (as in folliculitis) but may be sterile (as in pustular psoriasis)
I. SCALE: flake-like compacted desquamated layers of stratum corneum. Desquamation occurs when there are peeling sheets of scale following acute injury to the skin. e.g. psoriasis
J. TELANGIECTASIA: visible (and permanent) dilatation of small cutaneous blood vessels in the skin. Can be isolated lesions or part of a generalized disorder, such as ataxia telangiectasia.
K. VESICLE and BULLA: small (few mm) and larger (several cm) fluid-filled blisters respectively. Filled with clear fluid. e.g. pemphigoid
L. WEAL: an area of dermal oedema, usually white due to masking of local blood supply by fluid, e.g. nettle sting
TUMOR: A tumor is a solid mass of the skin or subcutaneous tissue; it is larger than a nodule.
Secondary Lesions
Secondary lesions may evolve from primary lesions, or may be caused by external forces such as scratching, trauma, infection, or the healing process. The distinction between a primary and secondary lesion is not always clear.
Primary lesions are physical changes in the skin considered to be caused directly by the disease process.
Types of primary lesions are rarely specific to a single disease entity.
A. BURROW: burrows are linear/curvilinear lesions produced by infestation of the skin and formation of tunnels (namely by the scabitic mite or by cutaneous larva migrans).
B. COMEDONE: a plug of keratin and sebum wedged in a dilated pilosebaceous orifice
C. MACULE: a circumscribed flat area of altered colour e.g. freckle. A macule greater than 1 cm. may be referred to as a patch.
D. PAPILLOMA: a projecting nipple-like mass e.g. skin tag
E. PAPULE: a discrete elevation of skin that may be changed in colour. Those arising from the subcutis may be felt rather than seen. Larger lesions (>1 cm) are referred to as nodules. Papules may have a variety of shapes in profile (domed, flat-topped, umbilicated) and may be associated with secondary features such as crusts or scales.
F. PETECHIAE and PURPURA: Petechiae are pinhead-sized flat macules of extravascular blood in the dermis.
Purpura are larger and may be palpable
Ecchymosis ('bruise') is where bleeding involves deeper structures
G. PLAQUE: solid, raised, flat-topped area of skin greater than 1cm in diameter. It is analogous to the geological formation, the plateau. e.g. psoriasis plaque
H. PUSTULE: circumscribed elevated lesions that contain pus. They are most commonly infected (as in folliculitis) but may be sterile (as in pustular psoriasis)
I. SCALE: flake-like compacted desquamated layers of stratum corneum. Desquamation occurs when there are peeling sheets of scale following acute injury to the skin. e.g. psoriasis
J. TELANGIECTASIA: visible (and permanent) dilatation of small cutaneous blood vessels in the skin. Can be isolated lesions or part of a generalized disorder, such as ataxia telangiectasia.
K. VESICLE and BULLA: small (few mm) and larger (several cm) fluid-filled blisters respectively. Filled with clear fluid. e.g. pemphigoid
L. WEAL: an area of dermal oedema, usually white due to masking of local blood supply by fluid, e.g. nettle sting
TUMOR: A tumor is a solid mass of the skin or subcutaneous tissue; it is larger than a nodule.
Secondary Lesions
Secondary lesions may evolve from primary lesions, or may be caused by external forces such as scratching, trauma, infection, or the healing process. The distinction between a primary and secondary lesion is not always clear.
- ATROPHY: Atrophy is thinning or absence of the epidermis, dermis or subcutaneous fat. Results in translucency e.g. excess topical corticosteroids
- CRUST: Crusting is the result of the drying of plasma or exudate on the skin. Crusting is different from scaling. The two terms refer to different phenomena and are not interchangeable. One can usually be distinguished from the other by appearance alone.
- ESCHAR: An eschar is a hard, usually darkened, plaque covering an ulcer implying extensive tissue necrosis, infarcts or gangrene.
- EXCORIATION: Excoriations are traumatized or abraded skin caused by scratching or rubbing.
- EROSION: Erosions are slightly depressed or denuded areas of skin in which part or all of the epidermis has been lost.
- FISSURE: A fissure is linear cleavage of skin which extends into the dermis.
- KELOIDS: Keloids are an exaggerated connective tissue response of injured skin that extend beyond the edges of the original wound.
- LICHENIFICATION: "Lichenification" refers to a thickening of the epidermis seen with exaggeration of normal skin lines. It is usually due to chronic rubbing or scratching of an area.
- SCAR: Scars are the permanent fibrotic changes that occur on the skin following damage to the dermis. Scars may have secondary pigment characteristics.
- ULCER: Ulcerations occur when there is necrosis of the epidermis and dermis and sometimes of the underlying subcutaneous tissue.
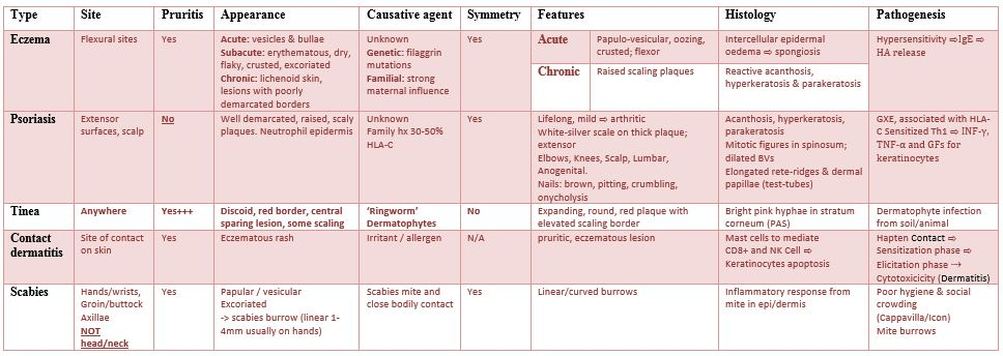
Recognise the differences in Eczema, tinea and psoriasis and other red rashes.
|
Eczema:
o Contact o Irritation o Seborrhoeic Dermatitis o Pomphylox o Discoid o Photosensitive o Varicose Potential Infx o Staphylococcus Aureus o Herpes Simplex (eczema herpeticum) o Molluscum Contagiosum o Streptococcus o Candida Pathogenesis: genetic defect affecting IL4 and IgE mediated immune reactions
Antigen exposure results in: o IgE antibody production o Release of Pro-Inflammatory Mediators o Erythematosus and Pruritus Management: Emollients, Mosturisers, Antiseptics, Wet Wraps, Coal Tar, Topical steroids - Finger Tip Unit for Steroids |
Tinea:
o Trichophyton o Microsporon o Epidermophyton Microsporon species are mainly caught from infected dogs or cats Trichophyton species are caught from animals
Microscopy of derm scrapping (specimen) looks for hyphae and culture - where the species can be identified) but culture often takes up to six weeks so one often has to start treatment without conformation of the Dx. Occurance
Different Types: o Tinea Corporis: Body and Limbs o Tinea Cruris: Groin area or young men o Tinea Pedis: Feet (Athletes Foot) o Tinea Capitis: Scalp 1. Diffuse hair loss with diffuse scaling and little or no inflammation or 2. Localised discoid hair loss often with very acute inflammation so looks like a weepy, boggy, crusty bald area (called a Kerion). o Tinea Unguiu: Nails, Asymmetric, Yellowish White, Thickening o Tinea Unguiu:: Immune system supression followed by thriving of dermatophytes (e.g. improper use of corticosteroids) |
Psoriasis:
Plaque Psoriasis: plaques are seen on the lower back, which are generally large well-demarcated plaques, usually on extensor surfaces. Guttate Psoriasis: seen on the upper back. Lesions generally appear as multiple small red raised scaly patches, usually all over the trunk. This condition is often seen in young people following a throat infection. Palmoplantar Psoriasis: yellowish / brownish sterile pustules over the palms and soles, easily confused with the vesicular stage of pompholyx eczema but usually not as itchy. Generalised Pustular Psoriasis: sudden onset of widespread areas of pustules over the trunk and limbs, often accompanied by severe systemic upset with pyrexia and arthralgia. Later the whole area can peel. Fortunately fairly rare as these patients are extremely unwell sometimes requiring intensive care. Erythrodermic Psoriasis: patients develop widespread red scaly skin often affecting the whole body. There is marked heat loss so these patients are at risk of hypothermia. They can also suffer excessive water loss so are at risk of dehydration. The hyperdynamic circulation can lead to high output heart failure. These patient general need urgent hospital admission. |
Describe the main symptoms of Eczema.
Definition/Description
Itchy, inflammatory dermatoses where the lesions are red, lichenified (thickened skin), often excoriated (scratched) and often flaky or cracked. The lesions often do not have well demarcated borders as they fade into the surrounding skin. Secondary infection with staphylococcus aureus is common causing the eczema plaques to develop yellowish crusting or weepy areas.
Epidemiology
Prevalence of 2.5% of Children worldwide
~10% of young adults worldwide
Classification:
Pompholyx eczema that affects palms and soles causing itchy vesicles that often brake down to thicken cracked palms and soles.
Eczema Herpeticum is secondary infection of eczema with herpes simplex virus. The patients are often children who develop vesicles and vesiculo-pustules over the eczema which evolve into small monomorphic crusty erosions. It can be localised or widespread, the patient can be very unwell with high fevers. If the lesions are widespread and the child very unwell they usually require admission for IV or oral aciclovir.
Black skin patients can develop papular eczema where there are numerous follicular papules often on a rather lichenified background.
Black skin patients often develop pigment changes, both darker and lighter called post inflammatory hyper / hypopigmentation
Discoid eczema are discrete circular patches of eczema usually not in flexural sites and can easily be misdiagnosed as Tinea (fungal infection/ringworm) The lower legs are a common site and it is more common in older patients.
Seborrhoeic eczema (aka seborrhoeic dermatitis) can affect babies as symmetrical red roughened plaques often with yellowish scale on the face (especially the eyebrows) and scalp (cradle cap), nappy area and flexural sites such as axillae and neck. It is not particularly itchy whereas in atopic eczema itch is a main symptom. In babies it is self limiting and usually resolves by the time the child is one year. Some of these babies will go on to develop classical atopic eczema but many do not. It can also affect adults particularly in sebaceous or hair bearing areas such as scalp (dandruff), eyebrows, around the nasal ala, the front of the chest and groin. The exact cause is unknown but it is thought that the fungus pityrosporum ovale (normal skin flora) reacts with sebum creating an irritant that leads to the clinical appearance of red scaly skin. In adults it tends to run a more chronic course. It is very common in patients with HIV who often have quite extensive seborrhoeic dermatitis
Itchy, inflammatory dermatoses where the lesions are red, lichenified (thickened skin), often excoriated (scratched) and often flaky or cracked. The lesions often do not have well demarcated borders as they fade into the surrounding skin. Secondary infection with staphylococcus aureus is common causing the eczema plaques to develop yellowish crusting or weepy areas.
Epidemiology
Prevalence of 2.5% of Children worldwide
~10% of young adults worldwide
Classification:
Pompholyx eczema that affects palms and soles causing itchy vesicles that often brake down to thicken cracked palms and soles.
Eczema Herpeticum is secondary infection of eczema with herpes simplex virus. The patients are often children who develop vesicles and vesiculo-pustules over the eczema which evolve into small monomorphic crusty erosions. It can be localised or widespread, the patient can be very unwell with high fevers. If the lesions are widespread and the child very unwell they usually require admission for IV or oral aciclovir.
Black skin patients can develop papular eczema where there are numerous follicular papules often on a rather lichenified background.
Black skin patients often develop pigment changes, both darker and lighter called post inflammatory hyper / hypopigmentation
Discoid eczema are discrete circular patches of eczema usually not in flexural sites and can easily be misdiagnosed as Tinea (fungal infection/ringworm) The lower legs are a common site and it is more common in older patients.
Seborrhoeic eczema (aka seborrhoeic dermatitis) can affect babies as symmetrical red roughened plaques often with yellowish scale on the face (especially the eyebrows) and scalp (cradle cap), nappy area and flexural sites such as axillae and neck. It is not particularly itchy whereas in atopic eczema itch is a main symptom. In babies it is self limiting and usually resolves by the time the child is one year. Some of these babies will go on to develop classical atopic eczema but many do not. It can also affect adults particularly in sebaceous or hair bearing areas such as scalp (dandruff), eyebrows, around the nasal ala, the front of the chest and groin. The exact cause is unknown but it is thought that the fungus pityrosporum ovale (normal skin flora) reacts with sebum creating an irritant that leads to the clinical appearance of red scaly skin. In adults it tends to run a more chronic course. It is very common in patients with HIV who often have quite extensive seborrhoeic dermatitis
List some of the factors possibly involved in the pathogenesis of atopic Eczema and the strength of evidence for or against their role in atopic eczema.
Atopic eczema:
- Often called endogenous eczema
- It occurs in those who are atopic (ppl who are predisposed to developing certain allergic and hypersensitivity reactions)
- It is common (5% of pop.)
Aetiology:
- Exact pathophysiology not fully understood, but there is initial selective activation of Th2-type CD4 lymphocytes in the skin which drives inflammatory process
- This precedes the chronic phase when Th0 and Th1 cells predominate
- In at least 90% of cases there is raised serum total IgE level
- It is a familial disease; if one parent has it, the risk for a child developing it is about 20-30%; if both parents have it, risk is greater than 50%
- There are abnormal skin-homing T cells in eczema (E) compared to controls, but the primary problem of E may be associated with deficient skin barrier function, thus suggesting that immunologic changes are secondary; loss-of-function mutations in the epidermal barrier protein filaggrin cause ichthyosis vulgaris but can predispose to atopic E in Caucasians
Exacerbating factors:
- Infection either in the skin or systematically can lead to an exacerbation, possibly by a superantigen effect
- Paradoxically, lack of infection (in infancy) may cause the immune system to follow a Th2 pathway an allow E to develop (called “hygiene hypothesis")
- Strong detergents, chemicals and even woolen clothes can be irritants and exacerbate E; severe anxiety or stress may also exacerbate E, as well as cat and dog fur (by both allergic and irritant mechanisms)
- Food allergens may also play role in triggering atopic E (i.e. dairy products)
Clinical features:
- Commonest presentation is of itchy erythematous scaly patches, especially in the flexures such as in front of the elbows and ankles, behind the knees and around the neck
- In infants, E often starts on the face before spreading to the body
- Very acute lesions may weep or exude and can show small vesicles
- Scratching can produce excoriations (traumatic lesions breaking epidermis and causing a raw linear area, a deep scratch), and repeated rubbing produces skin thickening (lichenification) with exaggerated skin markings
- In pts with pigmented skin, E often shows a reverse pattern of extensor involvement
- Also the E may be papular or follicular in nature, and lichenification is common
- A final problem in pigmented skin is of post-inflammatory hyper- or hypopigmentation which is often very slow to fade after control of the eczema
Associated features:
- Involvement of nail bed may produce pitting and ridging of nails
- In some atopic individuals the skin of upper arms and thighs may feel roughened due to follicular hyperkeratosis (keratosis pilaris)
- The palms may show very prominent skin creases (hyperlinear palms)
- There may be an associated dry fish-like scaling of the skin which is non-inflammatory and often prominent on the lower legs (ichthyosis vulgaris)
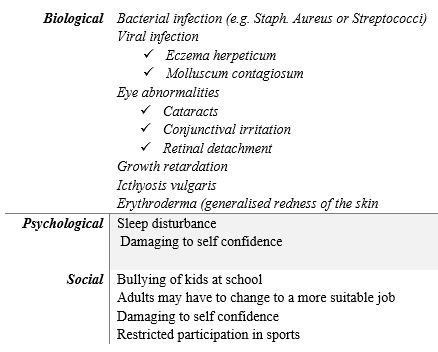
List the complications of Eczema.
Treatments for Eczema
Treatment of eczema and other red rashes uses a variety of methods; these include emollients, steroids, antibiotics and others
- Emollients: these are moisturizers and include aqueous cream, Diprobase, 50/50 SWP/LP, and Ung Merck
- Steroids are available as creams or ointments and are classified into 4 strengths; examples of these are mild (hydrocortisone), moderately potent (Eumovate), potent (Betnovate), and very potent (Dermovate); ointments are greasier and generally more effective in eczema than creams
- Antibiotics can be given as oral or topical preparations; they are used when rashes such as eczema develop a secondary bacterial infection or when the rash is due to bacterial infection; for instance, impetigo caused by Staph. aureus can be treated with Flucloxacillin, Erythromycin, and topical Abx, such as Fucidin, Fucidin H, and Betnovate C
- Wraps and Bandaging: Other treatments are generally used to stop irritation of the skin and avoid scratching; these include wet wraps and paste bandaging
Describe the main differential diagnoses for red scaly lesions.
Other
- Dermatitis subtype discoid or seborrhoeic
- Molluscum contagiosum (important) : viral; occurs mostly in children, infectious, if left untreated will resolve by itself in immunocompetent people. Round, firm, painless bumps ranging in size from a pinhead to a pencil eraser. If the bumps are scratched or injured, the infection can spread to surrounding skin.
- Lichen planus (itchy rash; can appear on the skin or inside the mouth. Sometimes, it appears in both places. Lichen planus can even change the way a person’s fingernails or toenails look. It also can appear on the genitals or a person’s scalp.
- Pityriasis rosea : common skin rash seen in young adults. Caused by a virus. The rash starts with a single large patch called a herald patch. After several days, more skin rashes will appear on the chest, back, arms, and legs.
- Secondary Syphilis
- Reiter’s syndrome : Reiter's syndrome is a form of arthritis that produces pain, swelling, redness, and heat in the joints. Inflammation sets off a disease process that involves the joints, eyes, urinary tract, and skin
- Discoid lupus: Discoid lupus erythematosus (DLE) is a chronic skin condition that appears as reddened scaly patches that develop in sun-exposed areas of the body
Outline how topical steroids are classified into 4 classes.
Class 1
Very potent (up to 600 times as potent as hydrocortisone)
Potent (100-150 times as potent as hydrocortisone)
Moderate (2-25 times as potent as hydrocortisone)
Mild
Very potent (up to 600 times as potent as hydrocortisone)
- Clobetasol propionate (Dermo Cream/Ointment
- Betamethasone dipropionate (Diproson OV Cream/Ointment)
Potent (100-150 times as potent as hydrocortisone)
- Betamethasone valerate
- Betamethasone dipropionate
- Diflucortolone valerate (Nerisone)
- Hydrocortisone 17-butyrate (Locoid)
- Mometasone furoate (Elocon)
- Methylprednisolone aceponate (Advantan)
Moderate (2-25 times as potent as hydrocortisone)
- Clobetasone butyrate (Eumovate)
- Triamcinolone acetonide (Aristocort)
Mild
- Hydrocortisone 0.5-2.5% (DermAid)
Revise the cell signaling pathway by which steroids have their effect.
Explain the risks of inappropriate topical steroid use.
They have can have side-effects ( these hormones are immunosuppressive etc, even if topical).
Systemic side-effects:
Localised adverse effects:
These include:
If potent steroids are required for control of inflammation for more than 7 days in a 5-week period, referral is recommended because of the risk of local side-effects.
Avoidance of infection may be promoted by steroid-antibiotic combinations (evidence is lacking), emollient antimicrobial preparations, not leaving tubs open, pump dispensers, and general hand hygiene measures.
Systemic side-effects:
- These are more likely with more potent steroids, larger quantities, more frequent application and where absorption is greatest (certain sites of the body and occlusion enhance absorption).
- Children, by virtue of skin type, surface area to weight ratio and disease severity are more at risk of systemic side-effects and should be monitored closely. The risk of growth restriction exists and growth should be monitored under specialist supervision where moderate strength steroids are required regularly.
Localised adverse effects:
These include:
- Spreading infection/opportunistic infection.
- Depigmentation.
- Skin thinning.
- Striae.
- Telangiectasia.
- Contact dermatitis.
- Perioral dermatitis.
- Acne.
- Acne rosacea.
If potent steroids are required for control of inflammation for more than 7 days in a 5-week period, referral is recommended because of the risk of local side-effects.
Avoidance of infection may be promoted by steroid-antibiotic combinations (evidence is lacking), emollient antimicrobial preparations, not leaving tubs open, pump dispensers, and general hand hygiene measures.
